

 PDF
PDF ePub
ePub Citation
Citation Print
Print


TO THE EDITOR: Therapy-related acute myeloid leukemia (t-AML) is a specific subtype of AML that accounts for 5% of secondary malignancies, among which therapy-related acute promyelocytic leukemia (t-APL) has been reported to be particularly rare, with a reported incidence rate of about 4.8% of all cases of acute promyelocytic leukemia (APL) according to a large Italian study [1]. However, an increase in the proportion of t-APL has been reported over time, with an incidence rate of up to 22% by the 2000s, owing to the increased use of chemocytotoxic agents or radiation therapy (RT) [2]. Cases of t-APL arising from plasma cell myeloma (PCM) are known to be rare, although they have been reported in a few instances associated with melphalan treatment. However, the effect of melphalan treatment alone on t-APL is obscure owing to the frequent use of combination therapy including topoisomerase II agents, other types of anti-cancer drugs, and/or RT [2345]. Herein, we report a very rare case of t-APL arising from PCM treated with melphalan only as a cytotoxic agent with a review of the literature.
A 71-year-old woman was admitted to the hospital for fever of unknown origin. The patient had a medical history of hypertension, osteoporosis, and iatrogenic Cushing's syndrome due to adrenal insufficiency. The initial complete blood count (CBC) showed a hemoglobin level of 9.5 g/dL, white blood cell count (WBC) of 5.41×109/L, and platelet count of 278×109/L. On peripheral blood smear, mild rouleaux formation was also observed. Diffuse osteoporosis and multiple compression fractures of the thoracolumbar spine were observed in a series of X-ray scans, and monoclonal gammopathy (Immunoglobulin [Ig] G kappa type, 1.5 g/L of M-protein in serum) was confirmed using serum immunofixation electrophoresis (IFE). Serum calcium and creatinine levels were normal. On bone marrow (BM) aspiration, 14.8% plasma cells with eccentric nuclei and basophilic cytoplasm were observed. The patient was diagnosed with PCM, and treated with 13 cycles of conventional melphalan and prednisolone (MP) therapy for 2 years.
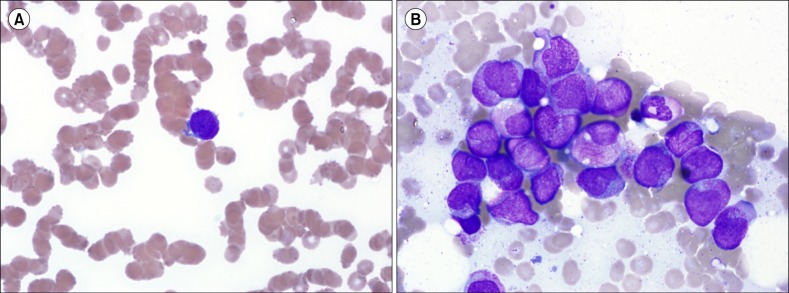
Pancytopenia was observed before the 14th cycle of MP therapy, and the patient was admitted for further evaluation. The CBC consistently revealed pancytopenia (hemoglobin level 9.7 g/dL, WBC 0.84×109/L, platelet count 38×109/L). As a peripheral blood smear showed 16% abnormal promyelocytes and immature cells (Fig. 1A), BM examination was conducted, followed by cytogenetic and molecular analyses using BM specimens. The BM aspirate showed 74% abnormal promyelocytes with bilobed nuclei, densely packed large granules, and Auer rods. The proportion of plasma cells was counted up to 2.6% (Fig. 1B). Some plasma cells were positive for kappa on immunohistochemical staining. Monoclonal peak was continuously observed on serum IFE, showing IgG and kappa type monoclonal gammopathy, 0.8 g/L of M-protein in serum. Chromosome analysis using a BM sample revealed a karyotype of 46, XX, t(15;17)(q22;q12) in 18 out of 23 metaphase cells examined (Fig. 2A). Fluorescence in situ hybridization (FISH) analysis using a dual color dual fusion PML/RARA probe showed 2 fusion signals in 176 out of 200 interphase cells; nuc ish (PML,RARA)×3 (RARA con PML×2)[176/200] (Fig. 2B). Multiplex reverse transcription (RT)-PCR analyses using HemaVision assay (DNA Technology, Aarhus, Denmark) confirmed the presence of PML/RARA gene rearrangement. The patient was diagnosed with t-APL and treated with all-trans retinoic acid (ATRA) immediately. Despite therapeutic efforts, the patient died 2 weeks later owing to cerebral infarction and subsequent sepsis.
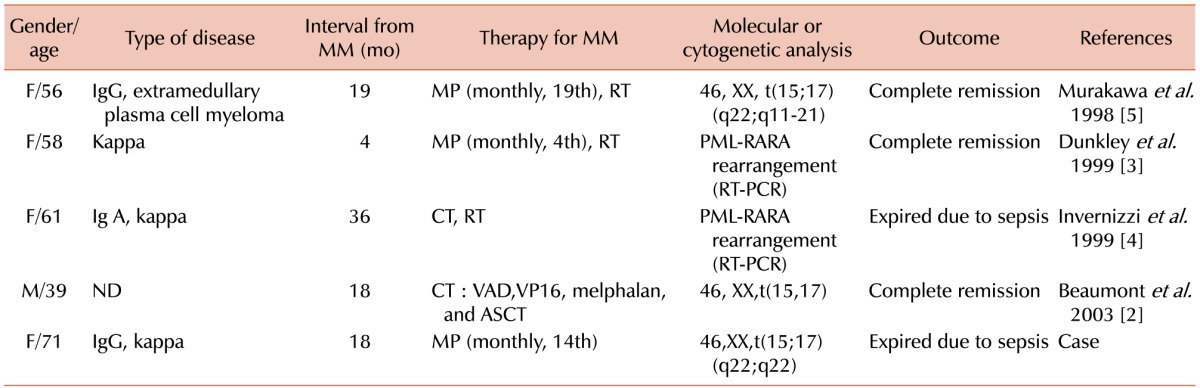
t-APL is closely related to topoisomerase II inhibitor administration [2]. The mechanism underlying the occurrence of t-APL associated with topoisomerase II inhibitor is the existence of “hot spots” in the PML and RARA genes with translocation breakpoints that are vulnerable to topoisomerase II inhibitor, and the concentrated position of such hot spots at a specific location [678910]. However, t-APL cases associated with the use of alkylating agents including melphalan had been rarely reported, and the mechanism underlying this association had not yet been elucidated. In order to search and compare similar cases, a search of the PubMed database (http://www.ncbi.nlm.nih.gov/pubmed/) was conducted. Cases of t-AML following treatment of PCM with alkylating agents including melphalan and/or RT were reported from time to time [11121314]. These cases usually corresponded to M1, M4 (myelomonocytic), or M6 under the past French-American-British (FAB) classification system; however, cases of M3 (Table 1), i.e., APL, were very rare [2345]. Two of 4 cases were treated with MP plus RT [35]. In the remaining 2 cases, melphalan and other cytotoxic agents without RT had been utilized in 1 case [2], and the name of the chemotoxic agent was not mentioned in the article for the other case, but RT was used [4]. Based on the patient characteristics summarized in Table 1, the disease course shows more aggressive pattern without a pre-leukemic phase or myelodysplastic syndrome, compared to other diseases related to alkylating agents. Since therapeutic combinations such as MP plus RT or various cytotoxic agents were utilized in the previously reported cases, the impact of various chemotherapy agents and RT was presumed to provoke t-APL. However, only MP therapy was administered in the present case. To the best of our knowledge, this is the first report of t-APL occurring during melphalan treatment without RT or any other chemotherapeutic agents, and implies the relationship between melphalan and t-APL in PCM. Further comparative studies between primary APL and t-APL arising from PCM could contribute to the improved understanding of the pathogenesis of t-APL.

 XML Download
XML Download