

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Infections with human parvovirus B19 are common and widespread; infections can cause a wide spectrum of clinical manifestations depending on the hematological and immunological status of the patients [1]. B19 infection may be asymptomatic or benign in immunocompetent individuals and may result in erythema infectiosum and arthropathy. Immunocompromised patients may become chronically infected [2]. Transmission of B19 occurs mainly through respiratory droplets, transfusion of blood or blood products, or transplacentally during maternal infection [34].
Parvovirus B19 has a marked tropism for erythroid progenitor cells and so can induce a temporary infection of the bone marrow, eventually leading to a sudden worsening of anemia, reticulocytopenia, and transient arrest in erythropoiesis in the bone marrow, which characterizes a transient aplasia crisis (TAC) [5678]. Patients with hematological disorders are at risk of severe clinical illness, especially in chronic hemolytic anemia such as thalassemia. In addition, patients with beta-thalassemia major are generally on a hyper-transfusion regimen; hence, they are at high-risk of acquiring transfusion-transmitted B19 virus and other transfusion-transmitted diseases. B19 infections have also been reported in recipients of Factor VIII concentrates, children with congenital coagulation defects, and multi-transfused hemophilia patients [91011].
Only one epidemiological study on human parvovirus B19 infection in Iranian patients with thalassemia has been reported, in which the prevalence of parvovirus B19 infection was compared between thalassemia major patients and healthy subjects [12]. The lack of sufficient information about the relationship between active B19 infection and thalassemia in Iran underscores the necessity to determine the rate of active B19 infection in thalassemia major patients. Monitoring of such high-risk groups is required for epidemiologic surveillance and disease-prevention measures. Here we report a molecular epidemiological study on B19 virus infection among beta-thalassemia major patients from Zafar Adult Thalassemia Clinic, Tehran, Iran. Diagnosis of B19 relies on serology and the detection of viral DNA [13]. We chose polymerase chain reaction (PCR) rather than serology as a detection method because of its high sensitivity and specificity [14], low cross-reactivity (especially with rubella and rheumatoid arthritis) [1516], and ability to detect both acute and persistent B19 infections [17].
MATERIALS AND METHODS
Study population
A total of 150 beta-thalassemia major patients from the Zafar clinic in Tehran were enrolled in this study between June and September 2016. All patients were undergoing transfusion regimens and were treated with regular transfusions of a single unit of packed red blood cells at each visit. The exclusion criteria included patients with other hemoglobinopathies such as sickle cell anemia and anemia due to other causes. Diagnosis of beta thalassemia major was based on peripheral blood smear examination and hemoglobin electrophoresis. This study followed the principles of the Declaration of Helsinki and was approved by the local ethics committee of the Kerman University of Medical Sciences, Kerman, Iran. The patients were informed about the current study, and informed consent was obtained from all of the patients prior to their enrollment.
Sample collection
After a positive diagnosis of beta-thalassemia major by a group of expert physicians, individual sampling took place. The sampling procedure was performed immediately after diagnosis for each patient. Five milliliters of whole blood were collected in a sterile tube containing ethylenediaminetetraacetic acid (EDTA) in order to separate the plasma. Afterward, the blood tubes were centrifuged for 5 min at 3,000 rpm. The plasma was collected in 1.5 mL microtubes and stored at −70℃.
Detection of viral DNA and genotyping
DNA was extracted using a commercial genomic DNA extraction kit (Bioneer, Daejeon, Korea). Specific primers and probe were designed and real-time PCR was performed with the program. The primers and TaqMan probe sequences were as follows:
Forward primer:5′-AATGCAGATGCCCTCCAC-3′ (position 1468–1485),
Reverse primer: 5′-ATGATTCTCCTGAACTGGTCC-3′ (position 1740–1760)
Probe: FAM-AACCCCGCGCTCTAGTAC-BHQ1 (position 1711–1728).
Samples positive for B19 were subjected to genotyping by real-time PCR using TaqMan master mix as follows: Pre-treatment (50℃, 2 min, l cycle), Initial denaturation (95℃, 10 min, 1 cycle), and annealing and extension (95℃, 15 sec, 45 cycles). A final melt step (60–95℃, 1 degree/cycle) and melting curve calculation was performed to determine the sample types. The human parvovirus B19 genotypes were determined based on melting curve analysis previously reported by Hokynar et al. [18].
RESULTS
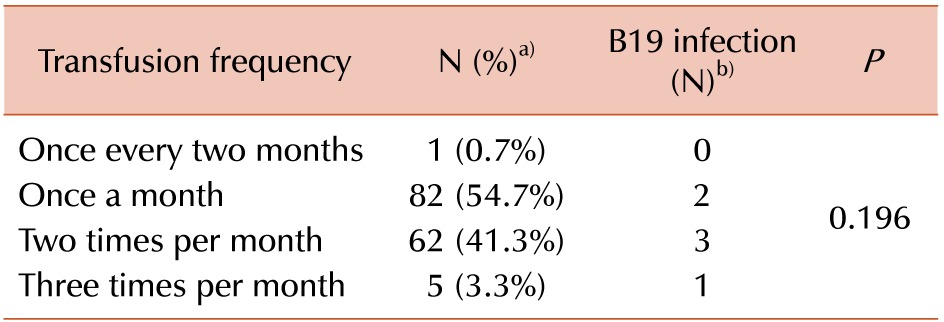
This study included 150 beta-thalassemia major patients with an equal distribution of genders (75 male and 75 female patients). The association of blood transfusion frequency and B19 infection is shown in Table 1. The age distribution of our cases included 53 patients (35.3%) between 26–30 years of age and 36 (24%) between 31–35 years of age. Patients 36–40 and 41–45 years of age comprised 10.7% and 5.3% of the study population, respectively. Cases under 20 and more than 45 years of age comprised 7.3% and 3.3% of all cases were, and 14% of the patients were between 20–25 years of age.
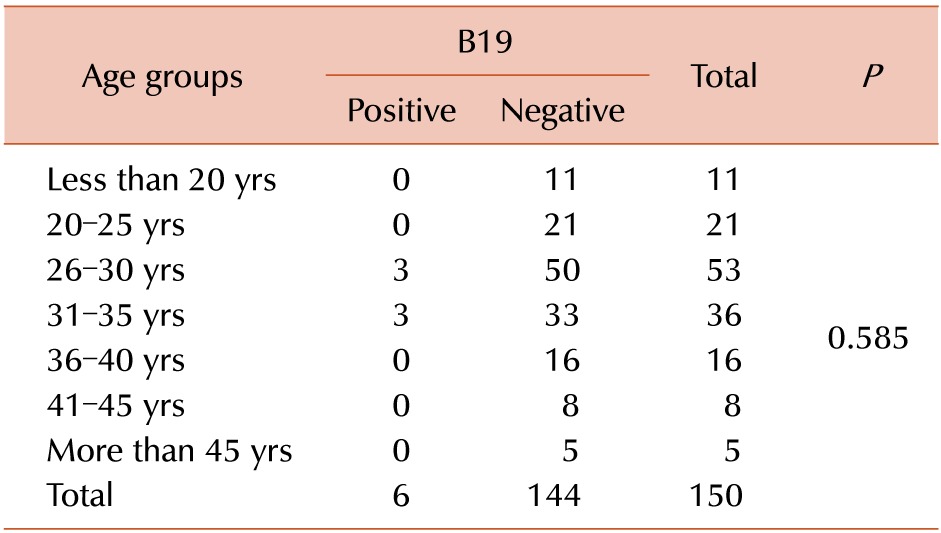
The real-time PCR detection of B19 DNA revealed six (4%) positive and 144 (96%) negative samples out of 150 subjects. In Table 2, the age distribution is shown based on human parvovirus B19 positivity. Three patients 26–30 year of age were positive for B19 virus, but 50 cases in this age group were negative. Among patients aged 31–35 years, three were positive for B19, while 33 were negative. Interestingly, no positive results were observed in the other age groups; based on our data, chi-square analysis showed a P-value of 0.585. Among 75 female patients, only one was positive and 74 were negative for human parvovirus B19. However, among 75 male patients, five were positive and 70 were negative for B19. In this study, all the genotypes were confirmed as type 1, with a P-value of 0.209.
DISCUSSION
Due to their regular transfusions, multi-transfused beta thalassemia major patients are the most susceptible population for transfusion-related infections, including human parvovirus B19 [3]. The objective of the present study was to evaluate the prevalence of acute B19 infections in Iranian patients with beta thalassemia major through the detection of its DNA in their sera by real-time PCR. Nikoozad et al. [12] reported a B19 DNA prevalence of 20% in 30 thalassemia major patients in Iran. However, our results show a reduction in prevalence (4%). This difference may be due to the fact that our results are based on the analysis of a larger study population. A small sample size will not provide a precise and reliable estimation of the prevalence and a larger sample size is needed to obtain a higher confidence level.
Several studies have reported the prevalence of human parvovirus B19 in patients with hematological disorders in different geographic regions worldwide. For instance, 60 thalassemia patients were examined between June 2001 and May 2002 in Thailand. The prevalence of anti-parvovirus B19 IgG and DNA were 38% and 13%, respectively, and anti-parvovirus B19 IgM was detected in 4% of patients positive for anti-parvovirus B19 IgG. Nucleotide sequencing and phylogenetic analysis of the NS1 gene indicated that these patients were infected with parvovirus B19 genotype I [19]. The incidence of B19 infection shows seasonal variation in temperate climates. B19 infections are more common in late winter and spring months in temperate climates, but cases may occur in any month [20]. In our study, all of the cases occurred during the summer, unlike the Thai study, a fact that may also contribute to the lower prevalence rate in our study.
Based upon DNA sequence analysis, parvovirus B19 can be divided into three main genotypes and sub-genotypes, which vary by up to 15% [21]. The clinical significance of these genotypes is unknown and requires further study. Genotype I is composed of all the prototype B19V isolates and is the most prevalent genotype worldwide whereas genotype II has been reported in several European countries including Finland and Germany, as well as the United States and Brazil [22]. Genotype III has been largely limited to Ghana, France, Brazil, and tropical areas in Africa [23]. For example, in one study in Brazil, the phylogenetic analysis demonstrated that all B19 isolates from patients with hemoglobinopathies were genotype I, confirming its widespread prevalence [24]. The connection between B19 genotypes and infection outcomes in patients with hemoglobinopathies is not yet known. Similarly, in our study, the phylogenetic analysis revealed genotype I in six B19-DNA-positive patients. We also observed a trend of increasing incidence of B19 infection with increasing transfusion frequency. However, due to the small sample size, the correlation between blood transfusion frequency and B19 DNA positivity was not statistically significant (P=0.196).
Epidemiological studies have shown that the prevalence of parvovirus B19 infection varies in different countries and societies around the world [252627]. The highest seroprevalence of IgG anti-parvovirus B19 was reported in Taiwan and Sweden [28]. In our study, 16.7% of parvovirus B19-positive patients were female, and 83.3% were male; this frequency differed from those of other countries such as Thailand and Brazil. In our survey, the mean age was 30.4 years. A similar study reported a mean age was 32 years, but another study reported 23.56 years of age, a mean age that was lower than ours. Slavov evaluated patients with sickle cell anemia and thalassemia in a similar survey in Brazil, 2012. Of 183 patients, 144 and 39 patients were diagnosed with anemia and beta-thalassemia, respectively. The prevalence of parvovirus B19 DNA in 28 patients with sickle cell anemia and six beta-thalassemia patients were 19.4% and 15.3%, respectively [24]. In a survey of patients five to 25 years of age in Iran from 2004–2005, parvovirus B19 IgG antibodies were detected in 83.5% of men and 88% of women. Moreover, 84.3% and 88% of the seropositive participants were from rural and urban areas, respectively [29]. In another study conducted at the Center for Special Diseases in Iran, the parvovirus B19 IgG prevalence in patients with hemophilia was 74%. In 2008, a study of Iranian blood donors found that no samples were positive for parvovirus DNA, suggesting the low risk of parvovirus transmission through blood cells [30]. Detection of specific IgM and IgG antibodies can help determine if the infection was recent; however, these antibodies can persist for months or even years after acute infection. This fact has limited the usefulness of this method because it is not possible to determine if the patient has an acute infection (which can put patients with hematological disorders at risk), or if the infection had occurred months prior. Therefore, as previous studies have demonstrated, seroprevalence is usually significantly higher than B19 DNA prevalence.
In this study, acute parvovirus B19 infections were detected at low rates among patients with beta thalassemia major. More number of comprehensive studies are needed in Iran in order to understand the actual B19 prevalence among patients with underlying hemolytic disorders including beta thalassemia. Until now, there have been no guidelines or protocols for B19 screening during blood donations. Preventive measures such as screening of donated blood must be implemented in order to avoid iatrogenic and nosocomial transmission of B19.
 XML Download
XML Download