

 PDF
PDF ePub
ePub Citation
Citation Print
Print


TO THE EDITOR: Interdigitating dendritic cell sarcoma (IDCS) is a very rare disease entity characterized by neoplastic proliferation of spindle-shaped cells with phenotypic features similar to those of interdigitating dendritic cell (IDC). To date, only about 100 cases of IDCS have been reported in English literature [1], and because of its rarity, the pathophysiology is not fully understood. Interestingly, IDCS has been reported to be associated with other malignancies, in particular lymphoid malignancies [23]. Traditionally, IDC has been recognized as a myeloid lineage due to its functional similarities to macrophages. Therefore, IDCS frequently occurring in patients with B-cell lymphoid malignancies is difficult to explain through the usual hematopoietic process, which is uni-directional and has irreversible lineage commitment. In this paper, we present a rare case of a patient who was diagnosed as NK/T cell lymphoma 19 months after achieving complete remission of IDCS with literature review.
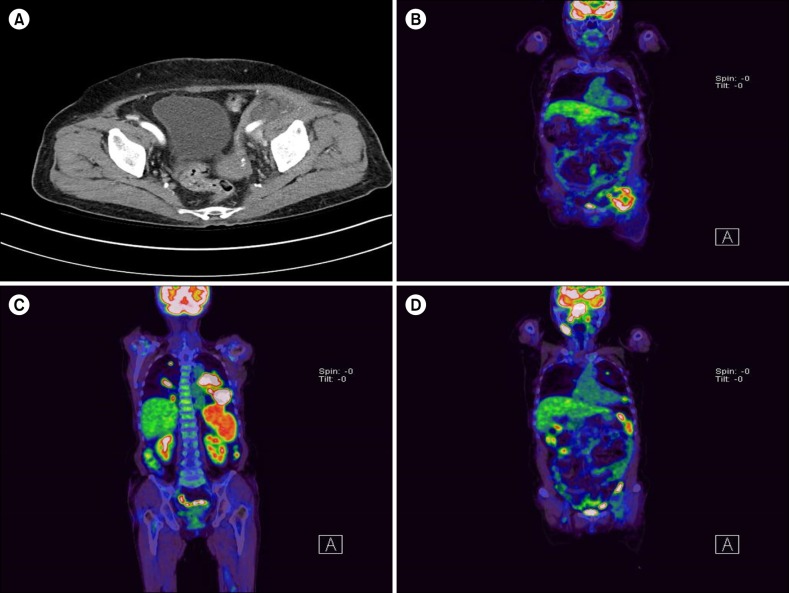
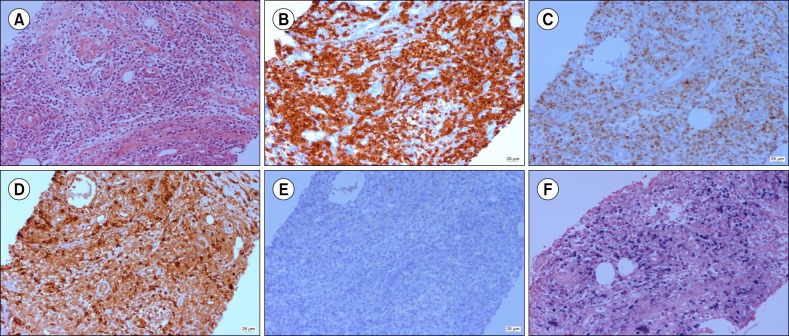
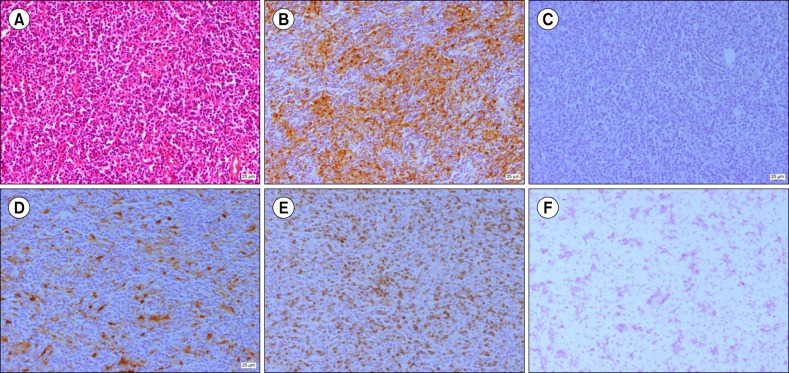
A 77-year-old female presented to our institution with palpable left lower quadrant abdominal mass in September 2015. Abdominal computed tomography (CT) scan showed a soft tissue mass near the left external iliac nodal area (Fig. 1A). Subsequent 18fluorodeoxyglucose-positron emission tomography (18 FDG PET)-CT showed high FDG uptake only on the same lesion (Fig. 1B). A core needle biopsy of the lesion revealed atypical T-cell proliferation with angiodestructive pattern (Fig. 2). Neoplastic cells were strongly positive for CD4, granzyme B, CD3, and CD8 but negative for CD20, CD1a, S-100, and CD56a. Fluorescent in situ hybridization of the biopsy specimen was positive for Epstein-Barr virus (EBV). These findings were consistent with NK/T cell lymphoma. Considering limited lesion, old age, and poor general condition of the patient, we performed radiation therapy for the abdominal mass. However, 1 month after completion of treatment, she complained of aggravated general condition with a febrile sensation. On sequentially performed PET-CT (Fig. 1C, D), disseminated FDG-avid masses were identified on the nasopharynx, lymph nodes in multiple areas, spleen, and both lungs, whereas the radiated abdominal mass regressed. Biopsy on the nasopharynx also revealed NK/T cell lymphoma. Despite Aspa-Met-Dex chemotherapy (dexamethasone 40 mg on days 1–4; high-dose methotrexate 3 g/m2 on day 1; and L-asparaginase 6,000 U/m2 on days 2, 4, 6, and 8 every 21 days), her condition drastically deteriorated only after the first cycle of chemotherapy, and she died of disease progression and pneumonia. Interestingly, 2 years earlier, she was diagnosed with IDCS after pathologic evaluation of newly developed cervical lymphadenopathy (Fig. 3). At that time, biopsy of the cervical lymph node showed S-100 and CD68 staining spindle- to ovoid-shaped cells intermingled with reactive T lymphocytes that are distinctively different from the pathologic finding of abdominal mass in this time. She received 6 cycles of ABVD chemotherapy (doxorubicin 25 mg/m2, bleomycin 10 mg/m2, vinblastine 6 mg/m2, and dacarbazine 375 mg/m2 on days 1 and 15 every 28 days) for IDCS and achieved complete remission. She has remained well for 19 months (Fig. 2B).
The World Health Organization classifies dendritic cells (DCs) into 4 types: follicular, interdigitating, Langerhans cell, and fibroblastic cells. DC neoplasms are classified based on those 4 types of normal counterpart. Among them, IDCs are primarily distributed in the thymus or T-cell zones of lymphoid organs where they are responsible for presenting various antigens on the cell surface to the T-cells of the immune system. As mentioned earlier, IDCS cases have been frequently reported to be accompanied by synchronous or metachronous lymphoid malignancies. To elucidate this unique phenomenon, a few putative mechanisms have been proposed. The cross-lineage “trans-differentiation” theory is among the most convincing concepts. In particular, several recent studies demonstrated a clonal relationship between a few indolent B cell lymphoma and IDCS that occurred synchronously or metachronously in the same patient by showing the presence of identical clonal immunoglobulin (Ig) gene rearrangement or showing that the Ig gene harbors the same molecular or cytogenetic abnormalities in 2 different malignancies [45]. Moreover, some studies supported the lineage plasticity of DC by showing an inheritance of B-cell or T-cell genotype in patients with histiocytic/DC malignancies [6]. Although we did not perform comparative molecular study including assessment of T-cell receptor gene rearrangement, the 2 different hematologic malignant cells in our case are less likely clonally related with each other because NK/T cell usually does not rearrange T-cell receptor gene [7] and most previously reported secondary IDCS cases occurred after or concurrently with lymphoid malignancies. Shared etiologic factors such as common genetic abnormalities or viral etiology between NK/T cell lymphoma and IDCS can be considered as another potential mechanism. In NK/T cell lymphoma, EBV has been recognized as a principal pathogenetic factor. By contrast, viral etiology such as EBV has not been supported for IDCS, although follicular dendritic cell sarcoma (FDCS) is known to be associated with EBV infection [1]. Recently, B-RAF V600E mutation has been shown to be associated with a subset of histiocytic/DC tumors. In particular, O'Malley et al. [8] reported a case of IDCS that harbored B-RAF V600E mutation and was combined with B-cell lymphoma. However, considering the low incidence of B-RAF mutation in NK/T cell lymphoma, the probability of the 2 hematologic malignancies being related with B-RAF mutation is low [9]. Although the above theories cannot be applied to our case, 1 potential mechanism is helpful to explain this unique phenomenon. Because DCs play a crucial role in introducing tumor antigens to immune cells, particularly naïve T-cells, a diminished immune response of DCs caused by malignant transformation may contribute to the occurrence of secondary malignancy [10]. Considering the temporal order of 2 malignancies in our case, this theory is more convincing. Also, IDCS being more frequently associated with secondary malignancies than other subtypes of DC/histiocytic tumors support this theory. FDCS, which are mainly involved in humoral immunity, are frequently associated with autoimmune disease rather than secondary malignancy. By contrast, IDCS are mainly involved in cellular immunity, which is required in antitumor immunity.
To the best of our knowledge, this is the first case in which IDCS and metachronous NK/T cell lymphoma were confirmed in 1 patient. Our case provides additional evidence supporting that patients with IDCS tend to have concurrent or metachronous malignancies. As such, more thorough cancer surveillance is necessary in patients with IDCS even after complete remission.
 XML Download
XML Download