

 PDF
PDF ePub
ePub Citation
Citation Print
Print


TO THE EDITOR: Combined factor V and VIII deficiency, a rare autosomal recessive coagulopathy, was first defined by Oeri et al. in 1954 [1]. Although it is seen worldwide, Mediterranean countries have higher prevalence rates [2]. The presentation varies from mild to serious bleeding symptoms such as easy bruising, menorrhagia, epistaxis, gingival bleeding, intramuscular bleeding, and post-operation or tooth extraction bleeding. Plasma levels of the two factors vary between 5% and 30% [3]. Bleeding episodes are treated with factor V replacement by using fresh frozen plasma, desmopressin, and factor VIII replacement with special factor VIII concentrates [4].
A 20-year-old woman consulted our outpatient clinic with a complaint of continuous bleeding after tooth extraction. The patient's history revealed that she had been having long-lasting bleeding episodes after a minor trauma, easy bruising, and menorrhagia after menstruation. She did not have other signs of bleeding such as melena, hematochezia, hemoptysis, hemarthrosis, petechiae, and ecchymosis.
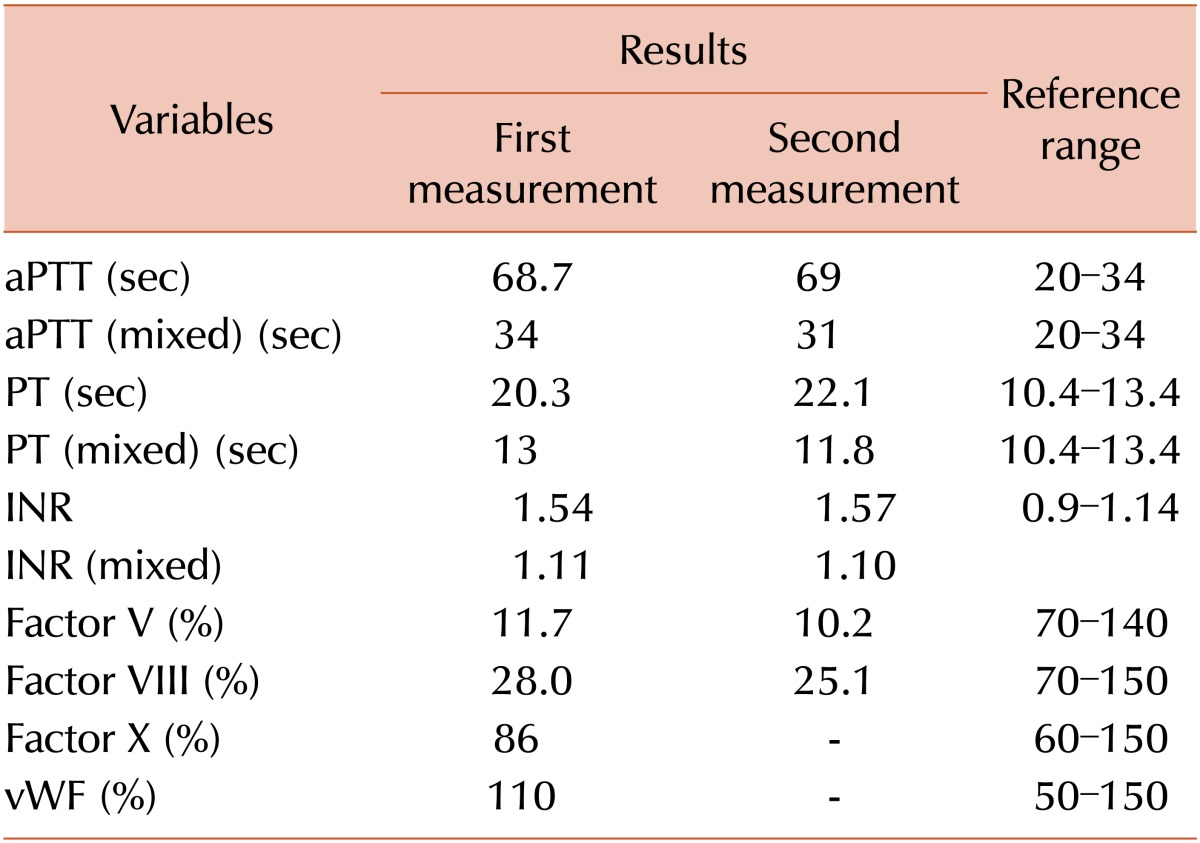
Her parents were not related, and her physical examination results and vital signs were normal. The total blood count was normal. Prothrombin time (PT) and activated partial prothrombin time (aPTT) were measured twice (18–20 sec and 65–68 sec, respectively; Table 1; normal reference range for PT, 10.4–13.4 sec; aPTT, 20–34 sec). Bleeding time was normal. aPTT and PT values were also normal after mixing the patient's plasma with a healthy plasma in a 1:1 ratio. Fibrinogen, factor VII, factor IX, factor X, and factor XI and von Willebrand factor levels were all normal. Factor V and VIII levels were measured twice, and both measured levels were low (11.7–10.2% and 28–25%, respectively; Table 1). According to these findings, the patient was diagnosed as having a combined factor V and VIII deficiency.
Combined factor V and VIII deficiency is known to be rare in the general population (1:1,000,000). However, it is seen more often in areas where consanguineous marriages are common [4]. The incidence of the disease was estimated to be 1 case per 100,000 individuals in the Middle Eastern Jewish and non-Jewish Iranian populations [5]. It is an autosomal recessively inherited disease and characterized by low levels of both factors V and VIII (generally between 5% and 20%) [6]. It is primarily caused by defects of the factor V and VIII coagulation secretion pathways, including lectin mannose-binding protein type 1 (LMAN1), which was previously called ERGIC-53, and multiple coagulation factor deficiency 2 (MCFD2) [7]. In these patients, the severity of hemorrhagic symptoms was found to be similar to that in patients with isolated factor V deficiency. Therefore, it can be suggested that combined factor V and VIII deficiency does not worsen bleeding severity [5]. Mild symptoms such as easy bruising, epistaxis, and gingival bleeding are frequently observed in these patients. Moreover, bleeding after tooth extraction, surgery, trauma, and menorrhagia and postpartum hemorrhage in females are not rare [58]. Gastrointestinal and central nervous system hemorrhages were reported in a few cases [28]. In our case, the patient was admitted with continuous bleeding after tooth extraction, and she had easy bruising, long-lasting bleeding after a minor trauma, and excessive bleeding during menstruation.
Factor V and VIII deficiency is characterized by normal platelet count and bleeding time but with prolonged PT and aPTT [9]. Similarly, the total blood count of our patient was normal, double measurements revealed prolonged PT and aPTT (18–20 sec and 65–68 sec, respectively), and bleeding time was normal. In combined factor V and VIII deficiency, regular prophylaxis is not required during bleeding episodes, and the patient is generally treated only when required. However, in case of recurrent hematoma and hemarthrosis, prophylaxis should be preferred [10]. The treatment of the bleeding is replacement of factor V and VIII. While factor V replacement therapy is administered by using fresh frozen plasma, factor VIII replacement therapy is administered by using special factor VIII concentrates (either plasma-originated or recombinant factor VIII products). Desmopressin can be administered in case of mild bleeding [4]. In our case, the patient was given fresh frozen plasma, and her bleeding stopped.
 XML Download
XML Download