

 PDF
PDF ePub
ePub Citation
Citation Print
Print


TO THE EDITOR: Translocations involving chromosome 7 rarely occur in AML and to date, nine cases with t(7;21) (p22;q22) involving ubiquitin specific peptidase 42 (USP42) at 7p22 and runt-related transcription factor 1 (RUNX1) at 21q22 have been reported as recurrent, semi-cryptic aberrations in AML. AML is associated with 5q abnormalities and hyperploidy [1234567]. In terms of t(6;7), this abnormality was reported in three AML cases as a mainline abnormality included in complex chromosomal abnormality [8910]. We report here a case of AML with a solitary t(6;7)(p21.3;p22) passenger translocation that developed at relapse after allogeneic hematopoietic stem cell transplantation (HSCT) in a patient with a normal karyotype at the initial diagnosis.
A 29-year-old man was admitted to the hospital in April 2013 due to a newly developed fever. His hemogram results were: WBC count, 193,460/µL; Hb, 8.5 g/dL; and PLT, 21,000/µL. His peripheral blood smear (PBS) showed many leukemic blasts (93%) and bone marrow (BM) aspiration exhibited proliferation of leukemic blasts (91.8%) that tested positive for myeloperoxidase (MPO) using cytochemical staining. The blasts also tested positive for CD34, CD13, CD33, CD117, HLA-DR, MPO, and CD7 using immunophenotyping. The HemaVision (DNA technology, Aarhus, Denmark) result was negative for all detectable fusion transcripts and conventional karyotype analysis showed 46,XY [20]. The FMS-like tyrosine kinase 3 internal tandem duplication (FLT3-ITD) and nucleophosmin (NPM1) mutation results were negative, but CCAAT enhancer binding protein alpha (CEBPA) tested positive for a double mutation [c.242_245dupTGTT in TAD1 domain and c.595_610del16 in TAD2 domain]. On the basis of these results, the patient was diagnosed with AML, not otherwise specified (NOS) and received induction chemotherapy with low dose cytarabine and idarubicin. After 3 months, he achieved complete remission and underwent allogeneic hematopoietic stem cell transplantation from a sibling donor. However, he developed chronic graft-versus-host disease (GVHD) of the liver in February 2014, and exacerbated hepatic GVHD in March 2015.
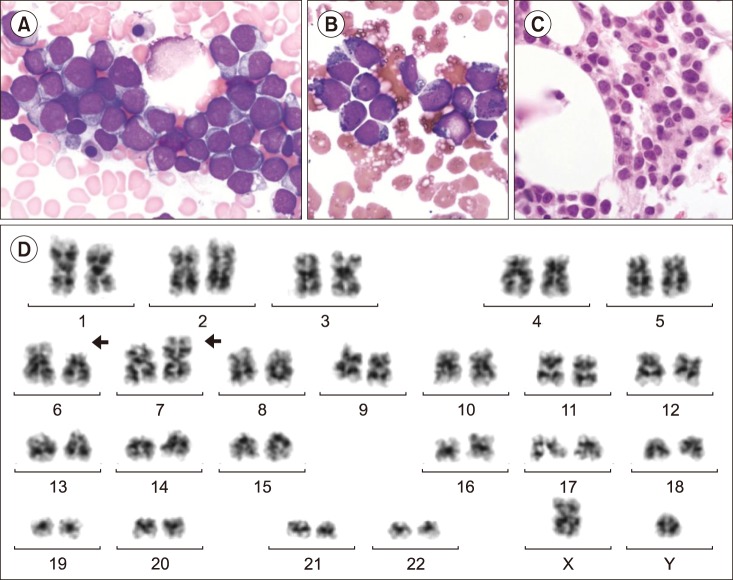
In April 2015, the patient was re-admitted to hospital due to general weakness, and his PBS showed leukocytosis, thrombocytopenia (WBC count 12,550/µL; Hb, 15.5 g/dL; and PLT, 40,000/µL), and infiltration of leukemic blasts (60%). BM aspiration showed proliferation of leukemic blasts (80.0%) (Fig. 1A); the blasts showed identical immuophenotyping results (positive for CD34, CD13, CD33, CD1117, HLA-DR, MPO, and CD7) to those obtained at initial diagnosis and they also tested positive for MPO using a cytochemical stain (Fig. 1B). The patient's BM biopsy showed normocellular marrow (cellularity of 40%) and diffuse infiltration of leukemic blasts (Fig. 1C). His HemaVision result was also negative and the FLT3-ITD, NPM1, and CEBPA mutation analyses demonstrated identical results to those obtained at the initial diagnosis. However, his karyotype result at relapse had changed to 46,XY,t(6;7) (p21.3;p22)[4]/46,XY[26], indicating the emergence of a solitary t(6;7)(p21.3;p22) clone with a frequency of 13.3% (Fig. 1D). The patient received induction chemotherapy with low dose cytarabine but he died 1 month after relapse due to exacerbated GVHD-induced liver failure.
The RUNX1/USP42 rearrangement in AML was predicted to encode a fusion protein retaining the runt homology domain (RHD); this domain is responsible for DNA binding and heterodimerization with core-binding factor β and the USP42 catalytic ubiquitin carboxyl terminal hydroxylase domain, which may result in the impairment of USP42 function and decreased p53 stability [111213]. Although our patient also showed development of translocation involving a 7p22 lesion, the other breakpoint was 6p21.3 and not 21q22, and both the clinical and cytogenetic features of our case were different from those in three previously reported AML cases with t(6;7) [8910]. These include occurrence in infants (two cases), the presence of t(6;7) as a mainline abnormality included in a complex karyotype (all three cases), and the absence of a breakpoint at 7p22 (two cases). Given that a small portion (13.3%) of analyzed cells showed t(6;7) and a high frequency of leukemic blasts (80.0%) at relapse, it is unlikely that the solitary t(6;7) (p21.3;p22) clone detected in our case has a pathological effect; it can be speculated that this would be a passenger translocation without gene fusions or pathobiological impacts that was retained by chance during cell division and clonal expansion. The identical immunophenotype and molecular mutation profiles at both, initial diagnosis and relapse would support this speculation.
However, we could not identify the translocated genes using metaphase FISH or RNA sequencing due to insufficient specimen quantity. Thus, we could not evaluate the genetic mechanism involving t(6;7) in AML, which is the main limitation of our report. Further studies focused on the identification of pathobiological mechanisms involving the t(6;7) clone in AML are required. In addition, since there was no report that showed t(6;7) in AML as a solitary major clone, we cannot evaluate whether the presence of t(6;7) in AML would be incidental or pathologic from the comparative analysis, and this would be an additional issue to be addressed.
When a new translocation of small clone size is developed at AML relapse after allogeneic HSCT, the possibility that this clone originated from the normal donor (so called constitutional translocation) should also be considered. However, a follow-up BM study of our patient after HSCT (in complete donor chimerism state) showed a normal karyotype, and this may be evidence that the minor t(6;7) clone detected in our case is not from the donor, but from the patient. Confirmation would require karyotype analysis using the fresh donor sample; however, we currently cannot perform this analysis, which is as an additional limitation of our study.
In conclusion, we report here a case with a solitary t(6;7)(p21.3;p22) passenger translocation that developed at relapse in an AML patient with a normal karyotype at the initial diagnosis. Genetic association between genes located in 6p21.3 and 7p22 in the pathogenesis of AML needs to be clarified in a future study.
 XML Download
XML Download