

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Lymphoplasmacytic lymphoma/Waldenstrom macroglobulinemia (LPL/WM) is a relatively rare subgroup of non-Hodgkin lymphoma (NHL). Differential diagnosis of LPL/WM from other NHLs is somewhat difficult, especially from marginal zone lymphoma (MZL) or B cell lymphoma with plasmacytic differentiation [12]. Recent studies have reported a high prevalence (80-100%) of the MYD88 L265P mutation in LPL/WM compared to a low prevalence in other NHLs; therefore, testing for this mutation could be of diagnostic value [345]. The incidence of LPL in Korea has been suggested to be low (0.8%) compared to that in western countries [6]. One recent study on Korean patients with LPL/WM also showed a relatively high prevalence (69%) of MYD88 L265P [7], whereas studies on other NHLs showed a low prevalence [89].
The detection methods for MYD88 L265P differed among different studies, and included conventional Sanger sequencing, allele-specific PCR (AS-PCR), and real-time PCR assays [410]. The specimens for molecular testing can be obtained from the lymph node, bone marrow aspirate, or peripheral blood samples. Since there is a high chance of inclusion of stromal and normal hematopoietic cells in such specimens, more sensitive methods will be required for accurate testing. In this study, we investigated the MYD88 L265P prevalence in Korean patients with LPL/WM and other B-cell NHLs using mutant enrichment 3'-modified oligonucleotide (MEMO)-PCR and sequencing, a sensitive technique with low false-positive rates [111213]. We observed a relatively high frequency of MYD88 L265P and determined the clinical utility of testing for this mutation.
Go to : 
MATERIALS AND METHODS
Patients and specimens
From a review of LPL/WL and other B-cell NHL cases diagnosed at the Samsung Medical Center between 2001 and 2014, we selected 97 cases with bone marrow involvement, including 28 LPL/WL and 69 other B-cell NHL cases. Patient demographics, clinical features, treatment histories, and hematologic, immunophenotypic, and cytogenetic findings were all comprehensively analyzed. To identify the deletion of 6q, we additionally performed fluorescence in situ hybridization (FISH) using the XL 6q21/6q23 probe (Metasystem, Altlussheim, Germany). For the evaluation of MEMO-PCR, samples were diluted with equimolar normal DNA to produce 1:1, 1:3, 1:5, 1:9, 1:17, 1:21, and 1:41 ratios of mutant DNA.
Mutant enrichment 3'-modified oligonucleotide–PCR (MEMO-PCR) and sequencing
DNA was extracted from bone marrow aspirate slides using the QIAamp DNA Blood Mini Kit (Qiagen, Foster City, CA, USA) after treating with proteinase K. To detect the MYD88 L265P by MEMO-PCR, we designed generic forward (5'-CAGGTGCCCATCAGAAGC-3') and reverse (5'-GAAGTTG GCATCTCCAGGAA-3') primers along with a blocking primer (5'-AAGCGACTGATCCCCATCAA-[C3 spacer]-3') employing a C3 spacer at the 3' end. PCR amplification was performed using these three primers (10, 10, and 50 pmol each, respectively), with the following amplification cycle: 94℃ for 5 min, 40 cycles of the main reaction (94℃ for 30 s, 59℃ for 30 s, and 72℃ for 60 s), and 72℃ for 7 min. Downstream sequencing analysis was performed using the BigDye Terminator Cycle Sequencing Ready Reaction Kit on the ABI Prism 3130 Genetic Analyzer (Applied Biosystems, Foster City, CA, USA). Principles of MEMO-PCR for MYD88 L265P detection are shown in Fig. 1 [12].
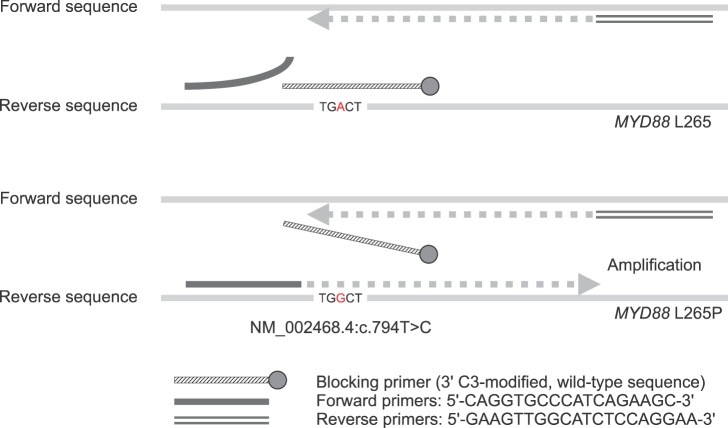 | Fig. 1Principles of MEMO-PCR for MYD88 L265P detection. Blocking primers, complementary to the normal sequence, anneal to normal DNA, hampering PCR amplification. In the presence of a missense mutation, the binding affinity of the blocking primers to the mutant DNA is decreased due to the mismatch, and therefore, amplification of the mutant DNA is markedly enhanced.
|
Statistical analysis
Statistical analysis was performed using PASW Statistics 20.0 software (IBM, Armonk, New York, USA). To compare the clinical parameters between MYD88 L265P positive and negative groups, we performed a chi-square test for categorical variables and a Mann-Whitney test or student's t-test for continuous variables. A P-value<0.05 was considered statistically significant.
Go to :
RESULTS
Clinical characteristics of LPL/WM
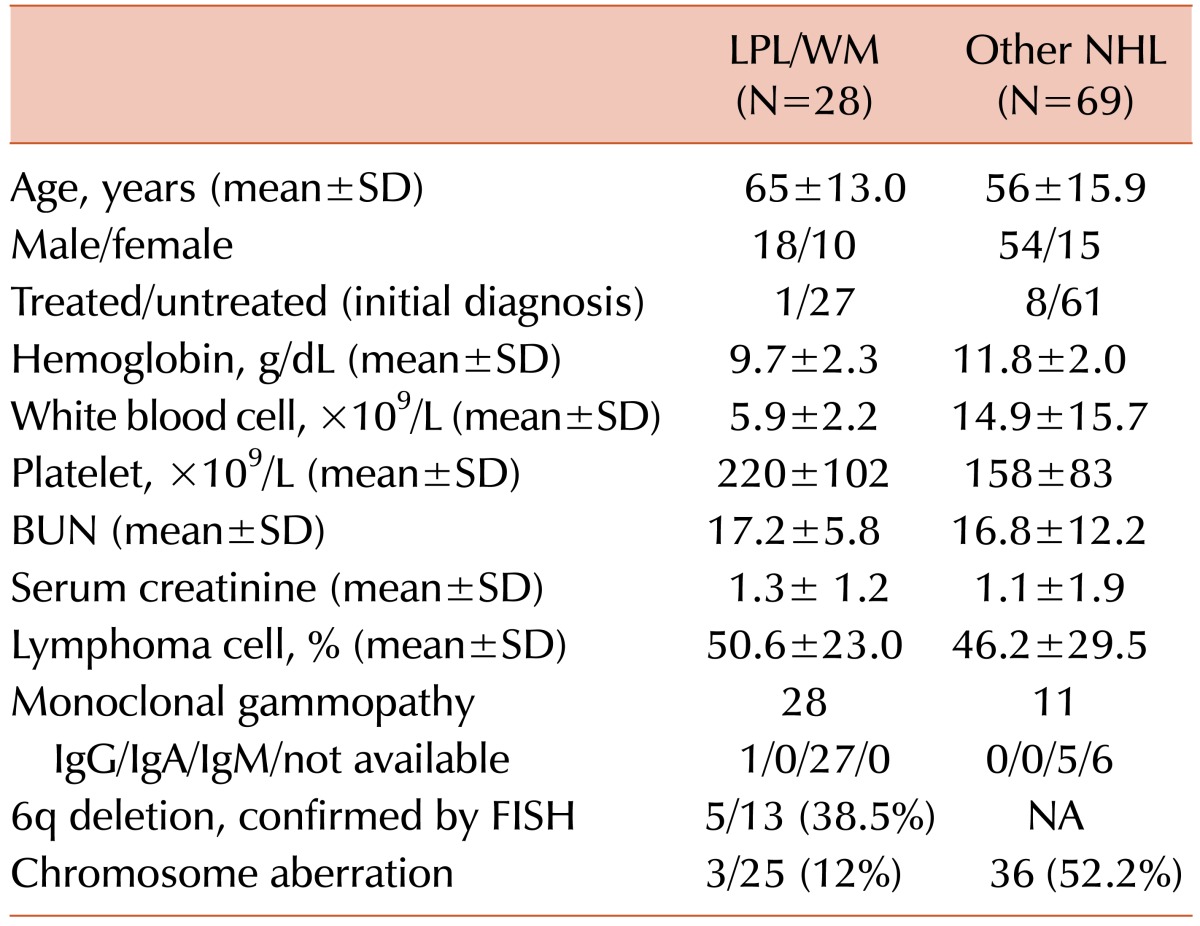
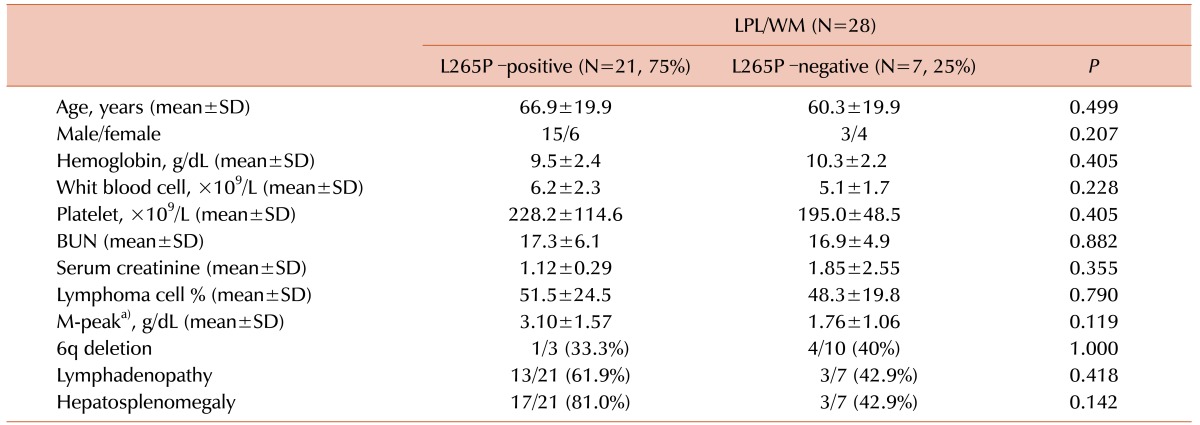
Patient demographics and clinical characteristics of cases are summarized in Table 1. The mean age was 65 years and the male/female ratio was 1.8:1. Patients generally had mild anemia (mean 9.7 g/dL) with variable white blood cell and platelet counts. All patients had IgM-type monoclonal gammopathies, except for one patient with IgG-type. Chromosomal aberration was detected in three of 25 patients analyzed (12%), including two complex karyotypes and one single balanced translocation. By FISH analysis, a 6q deletion was detected in 38.5% (5/13) of LPL/WM cases, suggesting that the deletion is cryptic. One case was CD5-positive (1/19, 5.3%). The positivity rate of CD23, CD25, and FMC-7 was 29.4% (5/17), 22.2% (2/9), and 50% (9/18), respectively.
Clinical characteristics of NHL
Demographic and clinical characteristics of the enrolled patients are summarized in Table 1. The mean age was 56 years and male/female ratio was 3.6:1. Patients generally had mild anemia (mean 11.8 g/dL) with variable white blood cell and platelet counts. Eleven patients had monoclonal gammopathies, which were most commonly of the IgM-type. Chromosome aberration was detected in 36 patients (52.2%).
Detection of MYD88 L265P
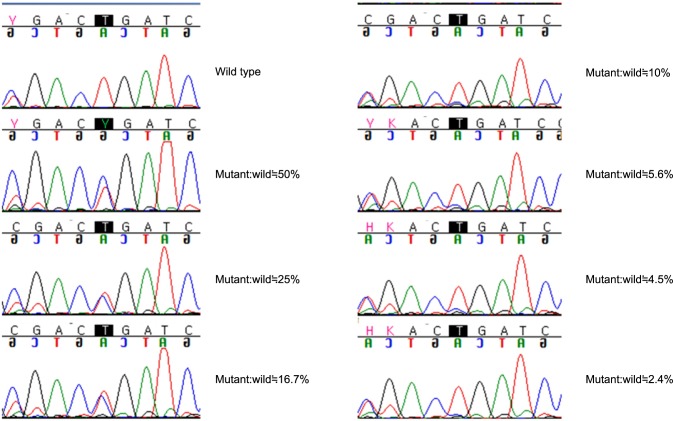
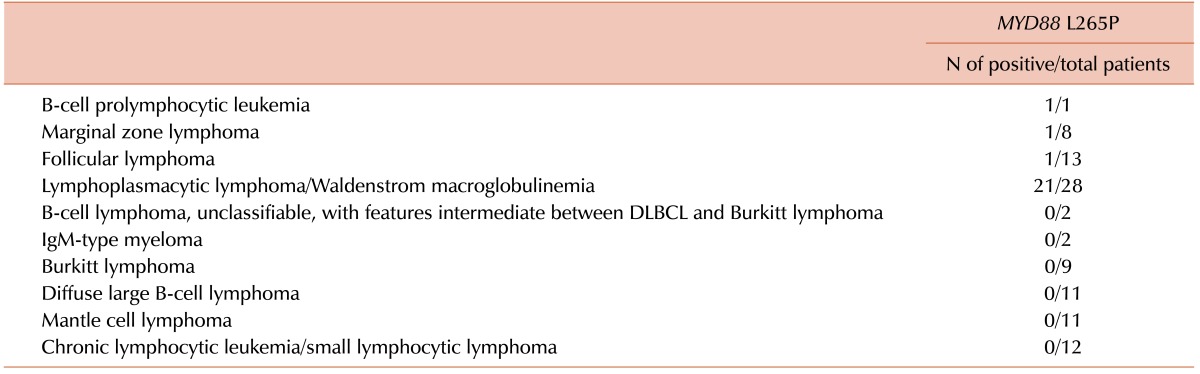
Using diluted samples, the sensitivity of MEMO-PCR was estimated to be approximately 10–16.7% (Fig. 2). By MEMO-PCR and sequencing of bone marrow aspirate specimens, MYD88 L265P was detected in 21 (75%) of 28 LPL/WM cases. In other B-cell NHLs, this mutation was detected in only three cases (4.3%), including B-cell prolymphocytic leukemia, marginal zone lymphoma, and follicular lymphoma (Table 2).
None of the clinical and cytogenetic parameters were significantly different between MYD88 L265P positive and negative groups (Table 3). Nonetheless, we observed relatively high serum paraprotein levels in the mutation-positive group compared to the wild type group (3.10±1.57 g/dL vs. 1.76±1.06 g/dL, respectively; P=0.119).
Go to :
DISCUSSION
We observed a high prevalence of the MYD88 L265P mutation in Korean LPL/WM patients, which was similar to results of previous studies [71014]. In 2012, Treon et al. initially described a high prevalence of MYD88 L265P in LPL/WM (91%) using whole genome sequencing [14]. They also developed real-time AS-PCR assays for sensitive detection and quantification of MYD88 L265P [10]. Other subsequent studies confirmed this high prevalence (over 90%) in LPL/WM and in IgM monoclonal gammopathy of undetermined significance (MGUS; up to 87% of cases) [515]. In addition, MYD88 L265P was considered a risk factor for progression to LPL/WM or other lymphomas in patients with IgM MGUS [151617].
MYD88 L265P can be detected in other B-cell NHLs; for example, approximately 30% of cases of the activated B-cell-like (ABC) subtype of diffuse large B-cell lymphoma (DLBCL) had the MYD88 L265P mutation [18]. Bonzheim et al. [19] have reported a high prevalence of MYD88 L265P (69%) in vitreoretinal diffuse large B-cell lymphomas. Cases of splenic marginal zone lymphomas and chronic lymphocytic lymphomas have also been reported to have MYD88 L265P although the frequencies are relatively low (10% and 4%, respectively) [10]. We also observed MYD88 L265P in three case of B-cell NHL, including B prolymphocytic leukemia, marginal zone lymphoma, and follicular lymphoma. These observations indicate that MYD88 L265P should not be considered an exclusive diagnostic marker of WM/LPL. Nonetheless, MYD88 L265P is relatively rare in marginal zone lymphomas, IgM myelomas, or chronic lymphocytic leukemia, of which the discrimination from LPL/WM is difficult. Therefore, the diagnostic utility of MYD88 L265P testing for differential diagnosis will be still valuable [1515].
Several studies have shown the association of the MYD88 L265 mutation with higher bone marrow tumor burden [3, 102021], serum paraprotein levels [1520], and probability of progression [151620]. In contrast, we could not identify any significant differences in laboratory and clinical parameters between MYD88 L265P positive and negative cases. This might be because of the small number of cases enrolled and the heterogeneity of clinical and pathological characteristics. Regarding cytogenetic abnormalities, no karyotype is known to be specific to LPL/WM. Loss of 13q14, 11q21-q22, and 6q23–q24 and gain of 3, 12, and 18 are reported to be common in LPL/WM [22] but these abnormalities are also common in other low-grade lymphomas such as MZL and CLL [2223]. We observed only three LPL/WM cases with chromosomal abnormalities by conventional chromosome analysis; however, a high frequency of 6q deletion (38.5%) was detected with FISH, which is in accordance with another study on Korean LPL/WM patients [7]. This report described an association between 6q deletion and MYD88 L265P mutation [7]. However, we failed to find a similar association; cases with a 6q deletion also had a high frequency of MYD88 L265P mutation.
For molecular testing, we used bone marrow aspirate slides instead of biopsy specimens from primary sites such as lymph nodes. Given that the detection method is sensitive, obtaining samples from bone marrow or peripheral blood specimens will be more practical and easier than performing biopsies on primary sites. One popular method for this purpose is AS-PCR, used in many studies for MYD88 L265P detection [410162425]. AS-PCR shows good sensitivity but sometimes suffers the drawback of high false-positive rates [1326]; therefore, we adopted a MEMO-PCR method with high specificity [111327] and confirmed that this technique could be efficiently used for the detection of MYD88 L265P mutations in LPL/WM and other B-cell NHLs.
Several limitations were encountered in this study. We did not perform extensive clinical and morphologic review of selected cases to differentiate LPL/WM from other lymphoma diagnoses. In addition, only a few cases of MZL or B cell lymphoma with plasmatic differentiation were enrolled in this study. The sensitivity of MEMO-PCR was insufficient to detect minimal mutant levels of MYD88 L265P. This low sensitivity could have caused the relatively low mutation prevalence (75%), when this parameter was compared to that in other studies (~90%). Therefore, clinical and laboratory differences, according to mutation status, might not have yielded statistical significance in this study. Further optimization of MEMO-PCR and sequencing might be required to increase detection sensitivity.
In conclusion, we observed a high prevalence of MYD88 L265P in LPL/WM and a low prevalence in other NHLs based on a series of Korean patients. Although several limitations were encountered in this study, our results demonstrate the diagnostic value of MYD88 L265P for differentiating B-cell NHLs.
Go to :
 XML Download
XML Download