

 PDF
PDF ePub
ePub Citation
Citation Print
Print


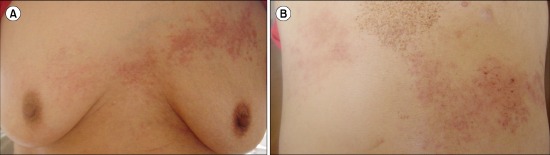
A 68-year-old female patient with IgG kappa-type multiple myeloma was treated with a bortezomib-based regimen. She had bilateral back pain 1 month after the chemotherapy. Because she had no skin lesions, we initially suspected, but did not find, a bone fracture. Two days later, we found eruptions with vesicles involving two different contralateral dermatomes on her chest and back where she had localized pain (A, B). We diagnosed herpes zoster duplex bilateralis based on Tzanck test results and treated the patient with intravenous acyclovir 750 mg/day for 6 days and immunoglobulin therapy. A few cases of herpes zoster duplex bilateralis have been reported, almost all of which were associated with some level of immunosuppression or cytotoxic therapy. In particular, several clinical trials have shown that a bortezomib-containing regimen can increase the risk of herpes zoster infection. Although herpes zoster duplex bilateralis is extremely rare, this case and illustration suggest a caution of herpes zoster infection when we treat multiple myeloma with a bortezomib-based regimen.
 XML Download
XML Download