

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The combination of rituximab with cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) has produced significant survival benefits, especially in elderly patients with untreated diffuse large B-cell lymphoma (DLBCL), compared to the CHOP regimen [1]. Although the immunochemotherapy improved clinical outcomes, some patients experience early refractoriness, unsatisfactory response, or relapse.
High-dose therapy (HDT) with autologous stem cell transplantation (ASCT) has become the standard of care for younger patients with chemosensitive relapsed non-Hodgkin lymphoma (NHL) and patients with primary refractory aggressive NHL [2]. In a recent study, the second-line age-adjusted International Prognostic Index (aa-IPI) accurately reflected prognosis in a group of patients with relapsed NHL [3]. The intergroup Collaborative Trial in Relapsed Aggressive Lymphoma evaluated salvage therapy regimens in HDT/ASCT-eligible patients, and the study identified several prognostic factors, including prior exposure to rituximab, early relapse (<12 months), and a secondary IPI of 2-3 [4]. In other studies, the use of 18-fluorine fluorodeoxyglucose (18F-FDG) positron emission tomography/computed tomography (PET/CT) in the relapsed setting was found to predict patient outcomes [56789].
Although HDT/ASCT is the standard treatment for improving clinical outcomes in relapsed patients, the treatment is associated with an extremely poor prognosis in elderly patients with relapsed or refractory DLBCL and for patients who are ineligible for HDT/ASCT. However, little is known regarding the prognostic factors that affect the clinical outcomes of patients.
The present study investigated the relationships and clinical value of several prognostic parameters and clinical outcomes in patients with relapsed or refractory DLBCL who are ineligible for HDT/ASCT.
Go to : 
MATERIALS AND METHODS
A retrospective review of records was performed at five medical centers in Korea (Pusan National University Hospital, Chonnam National University Hwasun Hospital, Seoul National University Bundang Hospital, Gachon University Gil Medical Center, and Pusan National University Yangsan Hospital). Patients who experienced relapse following R-CHOP therapy for DLBCL between 2006 and 2012 were included. Patients were excluded from the study if they had received additional therapies such as rituximab maintenance therapy after R-CHOP or underwent ASCT. During the period, all patients received treatment with the ifosfamide, carboplatin, and etoposide (ICE) regimen. The patients who received radiotherapy, and other types of salvage chemotherapy were excluded. This study was approved by the local Institutional Review Board.
Salvage therapy schedule
The ICE regimen was also administered in an inpatient setting. Ifosfamide was administered intravenously as a single dose of 5 g/m2/day on day 2 with mesna. Carboplatin was administered at a dose of 800 mg on day 2. Etoposide was administered intravenously at a dose of 100 mg/m2/day from day 1 to day 3. These two schedules were administered every 3 weeks.
aa-IPI
For each patient, the aa-IPI was assessed using data obtained immediately before the initiation of salvage therapy. The aa-IPI factors consist of elevated serum lactate dehydrogenase (LDH) levels above the upper limit of the normal range, Ann Arbor stage III or IV, and Eastern Cooperative Oncology Group (ECOG) performance status (PS) above grade 2. In the present study, each group was classified according to the sum of these risk factors as follows: the low-risk group had no risk factors, the intermediate-risk group had one risk factor, and the high-risk group had two or three risk factors.
18F-FDG-PET/CT scan and assessment of maximum standardized uptake value
All patients underwent an initial 18F-FDG-PET/CT scan before and after salvage therapy. All of the scans were analyzed using fusion software (Syngo, Siemens Medical Solutions, Malvern, PA, USA). By using the software package, the scans were evaluated in trans-axial, sagittal, and coronal views. Target lesions with a largest diameter >1 cm were identified on baseline 18F-FDG PET/CT scans. The maximum standardized uptake value (SUVmax) of each lesion was measured using the initial PET/CT scan. For each patient, the lesions with the greatest SUVmax were considered representative.
Response assessment and follow-up
After the diagnosis of relapse, the patients underwent a conventional re-staging work-up including a physical examination, complete blood cell counts and blood chemistry, CT (neck, chest, and abdominal-pelvic area), and PET/CT. The final response was assessed by using conventional CT and PET/CT. Bone marrow biopsy was performed only if it had been involved before salvage therapy. The response was assessed at 3 weeks after salvage therapy using the revised criteria of Cheson et al. [10].
Statistical analysis
Progression-free survival (PFS) was defined as the time between the beginning of salvage therapy until disease progression or death. Overall survival (OS) was defined as the time from the start of salvage therapy until death. The Kaplan-Meier method was used to estimate survival, and 95% confidence intervals (CIs) were calculated. Cox progression analysis was used to calculate the hazard ratio between the two arms. Receiver operating characteristic (ROC) curves were prepared to estimate the accuracy of predicting the ideal cut-off of SUVmax. The statistical analysis was conducted using SPSS software version 18.0 (SPSS Inc., Chicago, IL, USA). A P-value of <0.05 was considered significant.
Go to :
RESULTS
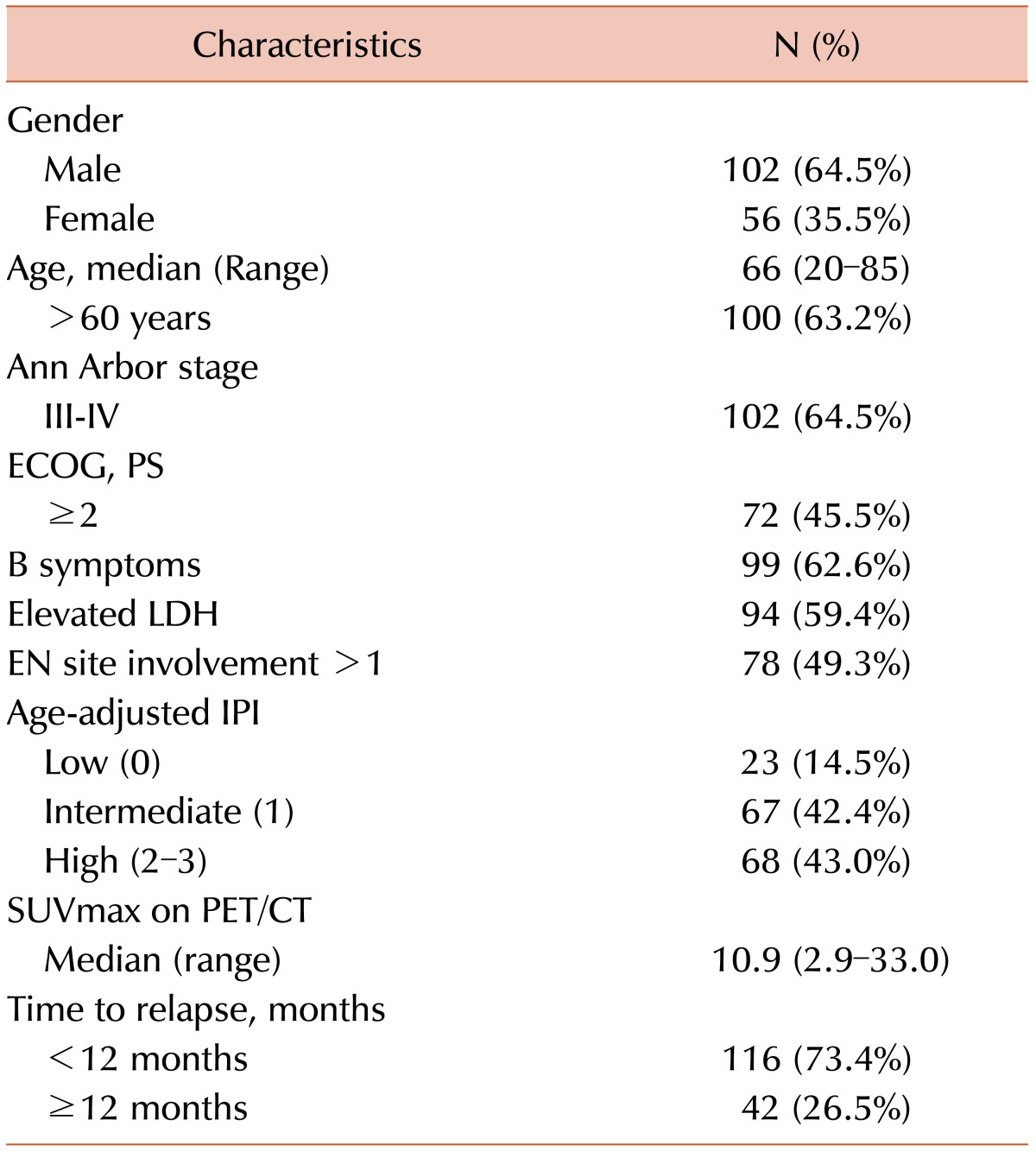
The baseline characteristics of the patients are summarized in Table 1. All 158 patients received ICE therapy. The male-to-female ratio was 102:56. The median patient age was 66 years (range, 20-85 years). One hundred patients (63.2%) were older than 60 years. In total, 102 patients (64.5%) had advanced disease (including stage III and IV), and 72 patients (45.4%) had an ECOG PS above grade 2. Ninety-nine patients (62.6%) had B symptoms, and the LDH level was elevated in 94 patients (59.4%). Forty-two patients experienced relapses that occurred 12 months after R-CHOP therapy (26.5%). Twelve patients (7.5%) achieved complete responses (CRs) after salvage therapy. The median follow-up duration was 32.6 months. During a follow-up period of 36.8 months, the PFS and OS rates were 26.9% and 33.5%, respectively, in the ICE group. The median number of chemotherapy cycles was 4.
Risk assessment using aa-IPI
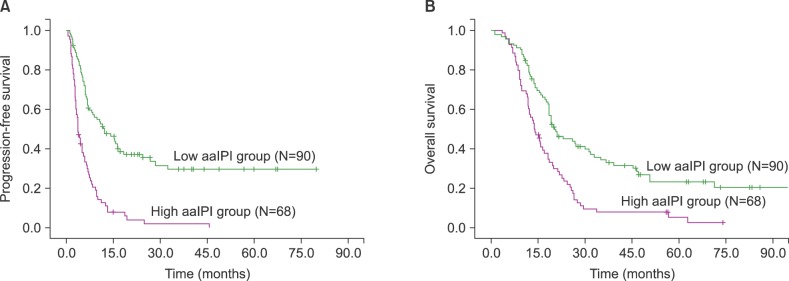
There were 23 patients in the low-risk group (0 aa-IPI risk factor). There were 67 patients in the intermediate risk group (1 risk factor), and 76 patients in the high-risk group (2-3 risk factors). Significant differences in PFS and OS were noted between the low- and high-risk groups (PFS, P <0.001 between the low- and high-risk groups; OS, P <0.001 between the low- and high-risk groups, Fig. 1A-B).
Risk assessment according to SUVmax at relapse
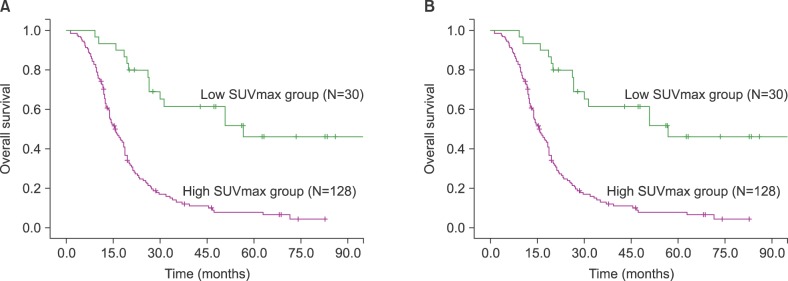
The median SUVmax was 10.9 (range, 2.9-33.0). The ideal cut-off for SUVmax was 6.0 according to ROC curve analysis. The area under the ROC curve of SUVmax was 0.811. The sensitivity and specificity were 90.1 and 73.1%, respectively. Depending on his or her SUVmax, each patient was categorized into either the low (<6.0) or high SUVmax group (≥6.0). According to this cut-off value, significant differences in survival were observed (P <0.001 for PFS and P <0.001 for OS, Fig. 2A-B).
Prognostic factors affecting clinical outcomes
To examine whether clinical outcomes were affected by various prognostic factors (age≥65 years, low aa-IPI, SUVmax <6.0, time-to-relapse >12 months, and CR status after salvage therapy), the factors were analyzed regarding their prognostic significance for salvage therapy.
In univariate analysis, a low aa-IPI (P <0.001 for PFS, P <0.001 for OS), SUVmax <6.0 (P <0.001 for PFS, P <0.001 for OS), time to relapse >12 months (P =0.025 for PFS, P <0.001 for OS), and CR status after the therapy (P =0.002 for PFS, P <0.001 for OS) were associated with both PFS and OS (Table 2).

Multivariate analysis revealed that a low aa-IPI (P <0.001 for PFS, P <0.001 for OS), SUVmax <6.0 (P <0.001 for PFS, P <0.001 for OS), and time to relapse ≥12 months (P <0.057 for PFS, P <0.001 for OS) were independent prognostic factors associated with favorable outcomes (Table 3).

Go to :
DISCUSSION
Few studies have been devoted to therapeutic options for patients with relapsed DLBCL who are ineligible for HDT/ASCT. It is well known that the prognosis is extremely poor with few therapeutic possibilities. The best therapeutic intervention is palliative chemotherapy together with other interventions to preserve a high quality of life. However, some subgroups of relapsed patients with low risk achieve a second good response and experience prolonged survival. Therefore, it is important to identify prognostic factors for predicting long-term outcomes in this population.
Several studies suggested the clinical value of certain prognostic factors including a tumor mass dimension larger than 10 cm, therapeutic regimens prior to ASCT, elevated LDH levels, short time to relapse, and an overall high disease burden [91011121314]. However, the widely accepted single prognostic model in the relapsed/refractory setting could not be generalized. A recent study illustrated the prognostic significance of aa-IPI based on the clinical data of patients with relapsed NHL who underwent HDT/ASCT [151617]. Guglielmi et al. also performed a retrospective analysis of aa-IPI factors for patients with relapsed DLBCL and identified relapse within 12 months of the initial diagnosis and aa-IPI factors as significant independent prognostic factors [18]. In addition, other clinical studies demonstrated the positive predictive value of aa-IPI [31920]. However, these results cannot be generalized to all patients with NHL because the aa-IPI factors were mostly focused on patients who underwent HDT/ASCT. Conversely, the present study was designed to evaluate the prognostic value of aa-IPI for patients with relapsed or refractory DLBCL who were ineligible for HDT/ASCT, and the data suggested that a low aa-IPI is associated with favorable outcomes for HDT/ASCT-ineligible patients.
Several research groups have investigated the use of 18F-FDG PET/CT to predict the outcomes of patients with relapsed or refractory NHL as well as newly diagnosed patients. In particular, it is well established that a CR on PET/CT or the negative conversion of FDG uptake after salvage therapy was associated with favorable outcomes [2122]. However, it is not known whether the degree of metabolic activity at the time of relapse influences clinical outcomes. In the present study, the clinical significance of the initial SUVmax and CR on PET/CT was evaluated in the relapsed setting. Interestingly, an initial high SUVmax at relapse was associated with an advanced Ann Arbor stage compared to a low SUVmax, and it had significant prognostic value for predicting poor clinical outcome. Meanwhile, the CR status did not have significance in the multivariate analysis. To confirm our result, additional clinical data are needed.
Recent studies demonstrated that SUVmax on pre-treatment 18F-FDG PET/CT was an important prognostic factor for patients with relapsed NHL who were treated with radioimmunotherapy [1011]. Salvage therapeutic regimens were used in patients with relapsed or refractory DLBCL. The present study only revealed clinical outcomes after ICE salvage therapeutic regimens. Therefore, further well-designed studies are needed to confirm our study.
In conclusion, the present study illustrated the prognostic significance of aa-IPI and SUVmax for patients with relapsed DLBCL who did not undergo ASCT. The aa-IPI and SUVmax were available to predict the survival outcomes in patients with relapse regardless of the use of salvage therapy. Although our study had limitations associated with its small sample size, the retrospective nature of its design, and the lack of rituximab assignment to salvage therapy, no prior study assessed the prognostic factors affecting patients with relapsed DLBCL who did not or could not undergo ASCT.
Go to :
 XML Download
XML Download