

 PDF
PDF ePub
ePub Citation
Citation Print
Print


TO THE EDITOR: Paraprotein is an abnormal immunoglobulin (Ig) or part of an Ig in the blood or urine that is produced by a clonal population of B cells and plasma cells. Production of a monoclonal Ig paraprotein is associated with various types of B-cell non-Hodgkin's lymphomas (NHLs). Paraproteinemia is associated with about 20% of patients with indolent types of NHL, whereas it appears to be rare in aggressive lymphomas [1]. Immunofixation (IFX) and conventional serum protein electrophoresis (SPEP) are useful tools to detect even low levels of monoclonal Igs. Herein, we report a case of diffuse large B cell lymphoma with a very high level of IgG kappa monoclonal gammopathy, which was rarely reported in the literature [2].
CASE
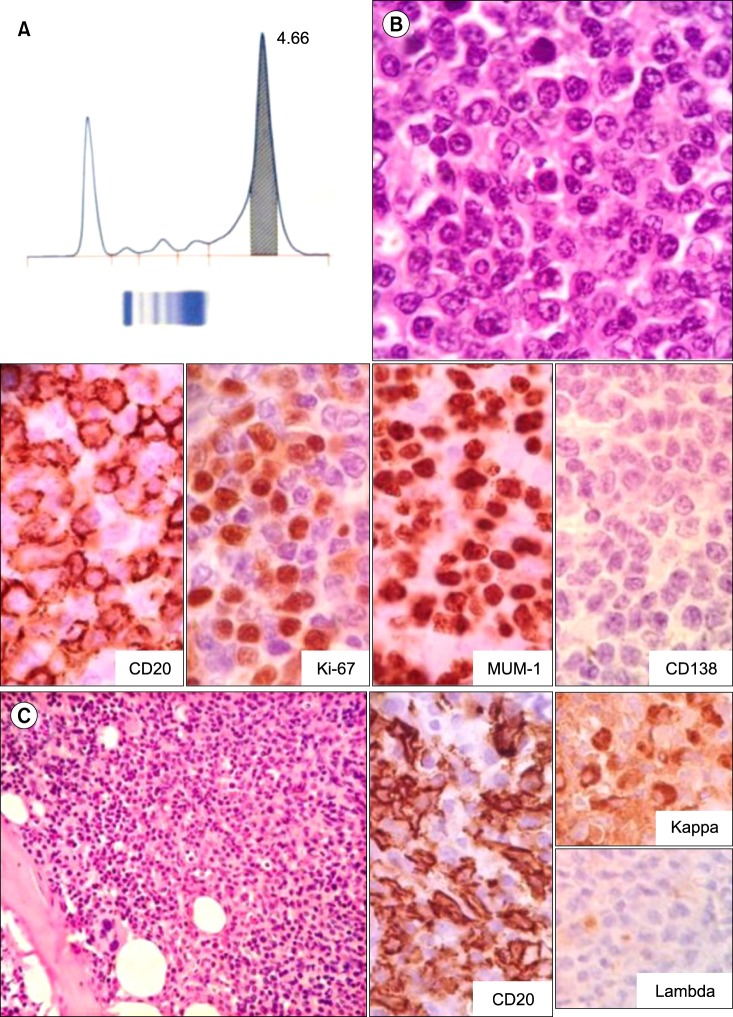
A 68-year-old man with a known case of rheumatoid arthritis presented with upper gastrointestinal bleeding. On examination, he was found to have axillary lymphadenopathy with splenomegaly. F-18 fluoro-D-glucose (FDG) positron emission tomography showed FDG avid bilateral axillary, external iliac, and inguinal lymph nodes and splenomegaly with diffusely increased FDG uptake. Hematological analysis showed hemoglobin to be 7.7 g/L; total leucocyte count, 8.9×109/L; and platelets, 80×109/L. Axillary lymph node biopsy showed sheets of large atypical lymphoid cells with irregular contours, brisk mitoses, and prominent nucleoli as well as perinodal spread. According to immunohistochemical analysis, these cells were positive for CD20 and MUM-1 and negative for CD3, CD10, Bcl-6, CD5, and cyclin D1. The Ki-67 index was found to be 70% (Fig. 1). A final diagnosis of diffuse large B cell lymphoma (DLBCL) was made, and bone marrow examination was performed for staging. Bone marrow preparation showed approximately 25% lymphoid cells including few abnormal forms, suggestive of lymphoma infiltration; this was confirmed on bone marrow biopsy by the presence of CD20 positive lymphoid cells in a diffuse and nodular pattern. Furthermore, plasma cell percentage was not increased and no monoclonal population was noted on biopsy, which was confirmed by immunohistochemistry for kappa and lambda light chains. SPEP revealed a monoclonal M band of 4.66 g/dL (Fig. 1), IFX identified this monoclonal protein to be IgG, kappa. A serum-free light chain assay showed the kappa level to be 325.98 mg/L, lambda 161.56 mg/L, and the ratio of kappa to lambda 2.0. A final diagnosis of stage IV DLBCL with paraproteinemia was made and the patient was started on R-CHOP therapy.
DISCUSSION
Paraproteinemia, or monoclonal gammopathy, is the presence of excessive amounts of paraprotein or a single monoclonal gammaglobulin in the blood. It usually occurs as a part of an underlying immunoproliferative disorder, such as leukemia, lymphoma, or plasma cell dyscrasia. Serum paraprotein levels in lymphoma patients are usually low and commonly associated with low grade lymphomas. Detection of monoclonal paraprotein using SPEP with quantitation of Igs and IFX should be included in the staging of lymphoma patients, as the presence of monoclonal gammopathy may influence prognostic stratification of these patients. Serum-free light chain assay is also a useful technique and may represent a significant prognostic marker for the detection of bulk and residual disease, both before and after treatment [3]. Further studies should be conducted to correlate the survival of these patients with the quantity and type of paraproteins and any requirement of a specific chemotherapeutic drug combination for improving overall survival. High M protein sometimes can lead to mislabeling of a case as plasma cell dyscrasia, delaying appropriate investigation. High paraprotein levels must not dissuade one from suspecting an underlying lymphoma, especially when relevant investigation for plasma cell dyscrasia is non-contributory
 XML Download
XML Download