

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acute lymphoblastic leukemia (ALL) is a neoplastic disease that results from multistep somatic mutations in a single lymphoid progenitor cell at one of several discrete stages of development. This disease causes leukemic cells to accumulate relentlessly because of their altered response to growth and death signals [1]. While ALL is mostly curable in children, similar progress in the treatment of ALL in adults has lagged behind, and some patients suffer from refractory or recurrent diseases that cannot be cured with conventional chemotherapy [2].
Therapeutic protocols used in ALL are widely variable. However, glucocorticoids (GC) are essential components in ALL treatment. GCs exert their antileukemic effects through reduction of cell proliferation, promotion of G1 cell cycle arrest, and induction of apoptosis. To induce antileukemic effects, GCs have to bind their intracellular receptor, which belongs to the nuclear hormone receptor superfamily. The ligand-receptor complex then translocates to the nucleus and transactivates or transrepresses, or both, GC responsive genes. Therefore, in oncology, GC function is mainly based on the induction of cell death [3].
The glucocorticoid receptor (GR) gene consists of 9 exons and is located on chromosome 5. Alternative splicing of the primary GR transcript can result in GRα and GRβ, and alternative splicing of the large exon 9 generates mRNA coding for GRα and GRβ. GRα has been the primary focus of research because of its predominant expression, ligand-binding properties, and transcriptional activity. However, GRβ does not bind GCs and is transcriptionally inactive [4]. Nonetheless, Oakley et al. demonstrated that GRβ, despite the fact that it is transcriptionally inactive, influences GC-mediated gene transcription [5]. The authors showed that GRβ was capable of binding and inactivating GRα, thus inhibiting signal transduction. More recently, a third splice variant of the GR, GRγ, was identified. GRγ was produced as a result of alternative splicing and retains 3 base pairs (bp) from the intron separating exons 3 and 4. As a consequence, an additional amino acid (arginine) is located between the 2 zinc fingers of the DNA-binding domain [6].
The GR gene is also named nuclear receptor subfamily 3, group C, member 1 (NR3C1). There are 3 known polymorphisms in the GR gene: Bcl I, N363S, and ER22/23EK [7]. The Bcl I polymorphism consists of a C to G substitution (TGATCA to TGATGA) and is located 646 bp downstream from exon 2 [8]. The N363S polymorphism results in an asparagine to serine substitution at codon 363 of exon 2. The ER22/23EK polymorphism consists of 2 linked single-nucleotide mutations in codons 22 and 23 in exon 2 of NR3C1 causing an amino acid change from arginine to lysine. Research regarding the impact of these polymorphisms suggests that the ER22/23EK polymorphism results in decreased sensitivity to GCs whereas the 2 other polymorphisms (N363S and BclI) have been associated with increased GC sensitivity [9].
The aim of this study was to evaluate the distribution of the 3 most prominent GR gene polymorphic variants (BclI, N363S, and ER22/23EK) among controls and Philadelphia-negative adult ALL patients as well as the relationship between these variants and GC sensitivity. In addition, we aimed to investigate the impact of pretreatment GR mRNA isoform expression on GC sensitivity as well as the response to induction chemotherapy in study participants. To our knowledge, this study is the first of its kind among adult ALL patients.
Go to : 
MATERIALS AND METHODS
Patients
The present study examined 52 newly diagnosed Philadelphianegative adult ALL patients who presented to the hematology department at the Alexandria University Medical Research Institute and the Mostafa Kamel Military Hospital in Alexandria. Patients were excluded if they had a prior malignancy or comorbid organ function abnormality. Patients were diagnosed and classified according to the morphological and immunophenotypic characterization of blast cells in the bone marrow. Cytogenetic studies were performed for all patients. Informed consent was obtained from all patients. Thirty apparently healthy age- and sex-matched volunteers were included as controls.
All patients completed a detailed history and a thorough clinical examination. Chemotherapy was given according to the Group for Research on Adult Acute Lymphoblastic Leukemia (GRAALL) 2003 protocol [10]. Peripheral blood samples were collected from participants upon diagnosis and before starting therapeutic measures. A 10 mL venous blood sample was drawn into 2 ethylenediaminetetraacetic acidcontaining sterile vacutainers. Patients were followed up for a median of 24 months (range, 5 to 40 mo) and event-free survival was calculated.
Response criteria
Corticosteroid sensitivity was defined as a peripheral blood blast cell count <1,000/µL after the 7-day corticosteroid prephase. However, corticosteroid sensitivity could not be examined in 3 patients who had a pretreatment peripheral blood blast cell count <1,000/µL. Chemotherapy sensitivity was defined as a bone marrow blast cell percentage less than 5% after the first week of chemotherapy [11]. Poor early responders were defined as patients with corticosteroid-resistant and/or chemotherapy-resistant ALL. Achievement of complete remission was evaluated according to the standard criteria [12].
Risk classification and stratification
Baseline high-risk factors included having a white blood cell (WBC) count ≥30×109/L for B-lineage ALL or >100×109/L for T-lineage ALL, an early T-cell phenotype, clinical and/or morphologic central nervous system (CNS) involvement, t(4;11) or t(1;19) translocation, hypodiploidy, -7 or +8 [10]. All patients with at least 1 baseline high-risk factor were classified in the high-risk ALL subgroup. All other patients were in the standard-risk ALL subgroup.
Polymerase chain reaction-restriction fragment length polymorphism of the GR gene
Genomic DNA was extracted using a genomic DNA purification Kit (Fermentas, USA) according to the protocol supplied by the manufacturer. Polymerase chain reaction (PCR) amplification of DNA segments containing the polymorphic sites was carried out using primer sequences (Table 1) and the PCR reaction mixture described previously [13]. The PCR protocol included denaturation at 95℃ for 5 minutes followed by 30 cycles of denaturation at 94℃ for 1 minute, annealing at 55℃ (except for N363S polymorphism at 51℃) for 1.5 minutes, extension at 72℃ for 1.5 minutes, and a final cycle at 72℃ for 5 minutes.

A restriction fragment length polymorphism analysis was performed to determine GR gene polymorphisms as described previously [71314]. To determine BclI polymorphism genotypes, 20 µL of relevant PCR product (335 bp) was digested by 20 units of BclI restriction endonuclease (Sigma-Aldrich, UK) for 1.5 hours at 50℃. The DNA fragments were separated on 2% agarose gel electrophoresis and visualized by ethidium bromide staining. The CC genotype produced 2 bands (117 and 222 bp), the CG variant gave 3 fragments (117, 222, and 335 bp), and the GG genotype remained undigested (335 bp).
To determine N363S polymorphism genotypes, 20 µL of relevant PCR product (248 bp) were digested with 1 unit of Tsp509I restriction endonuclease (Sigma-Aldrish, UK) for 1.5 hours at 65℃. Fragments were visualized by ethidium bromide staining after electrophoresis on agarose gel 3%. Digestion produced 3 fragments of 19, 95, and 134 bp (wild type allele, N363N) or 2 bands of 95 and 153 bp (heterozygous mutant allele, N363S) (Fig. 1).
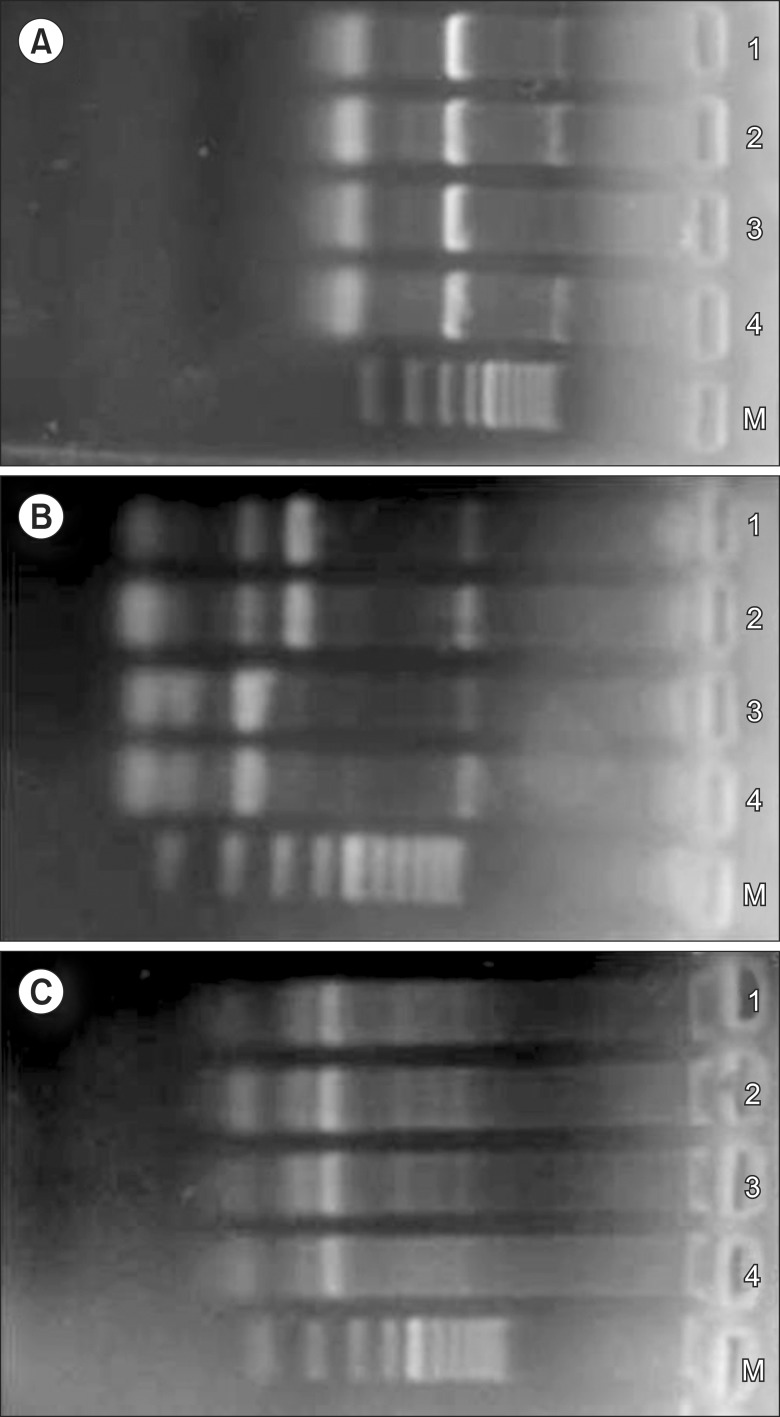 | Fig. 1
(A) Lanes 1-4 represent polymerase chain reaction (PCR) products for BclI polymorphism from 4 acute lymphoblastic leukemia (ALL) patients (335 base pairs (bp)). (B) Restriction fragment length polymorphism-digested PCR products for BclI polymorphism from ALL patients. Lanes 1 and 2 represent restriction fragments of PCR products for ALL patients with the CC genotype (222, 117 bp). Lanes 3 and 4 represent restriction PCR products for ALL patients with the CG genotype (335, 222, 117 bp). (C) Lanes 1-4 represent PCR products for N363S polymorphism from ALL patients (248 bp). Lane M represents the 100 bp ladder marker.
|
The ER22/23EK polymorphism genotypes were determined by digesting 20 µL of relevant PCR product (482 bp) with 1.25 units of MnlI restriction enzyme (Sigma-Aldrich, UK) at 37℃ for 1.5 hours. Fragments were visualized with ethidium bromide on a 2% agarose gel. Endonuclease digestion yielded fragments of 142 and 163 bp for the wild type allele (ER22/23ER genotype) while the heterozygous allele (ER22/23EK genotype) appeared as 3 bands of 142, 163, and 177 bp, and the homozygous allele (EK22/23EK genotype) gave 163 and 177 bp fragments.
Quantitative real-time PCR analysis of pretreatment GR isoform expressions
Peripheral blood mononuclear cells from patients and controls were isolated using Ficoll gradient centrifugation (1.077 g/mL). Total RNA was extracted using the RNeasy RNA extraction Mini Kit (Qiagen, USA). The extracted RNA was reversely transcribed using the QuantiTect Reverse Transcription Kit (Qiagen, USA) according to the manufacturer instructions. The GR α, β, γ primers and glyceraldehyde-3-phosphate dehydrogenase were designed, and the real-time PCR reactions were performed according to the Koga protocol [15]. The threshold cycle (CT) was used to calculate the mRNA expression levels of the PCR targets. The 2-ΔΔCT method was used for relative quantification [16].
Statistical analysis
Data were fed to the computer using IBM SPSS software package version 20.0. Qualitative data were described using numbers and percents. Comparisons between different groups regarding categorical variables were tested using a chi-square test. When more than 20% of the cells had an expected count less than 5, a Monte Carlo correction was used. Parametric tests were applied for normally distributed data, while nonparametric tests were used for abnormally distributed data. Significance of the obtained results was judged at the 5% level. Kaplan-Meier survival estimates and log rank P values were utilized.
Go to :
RESULTS
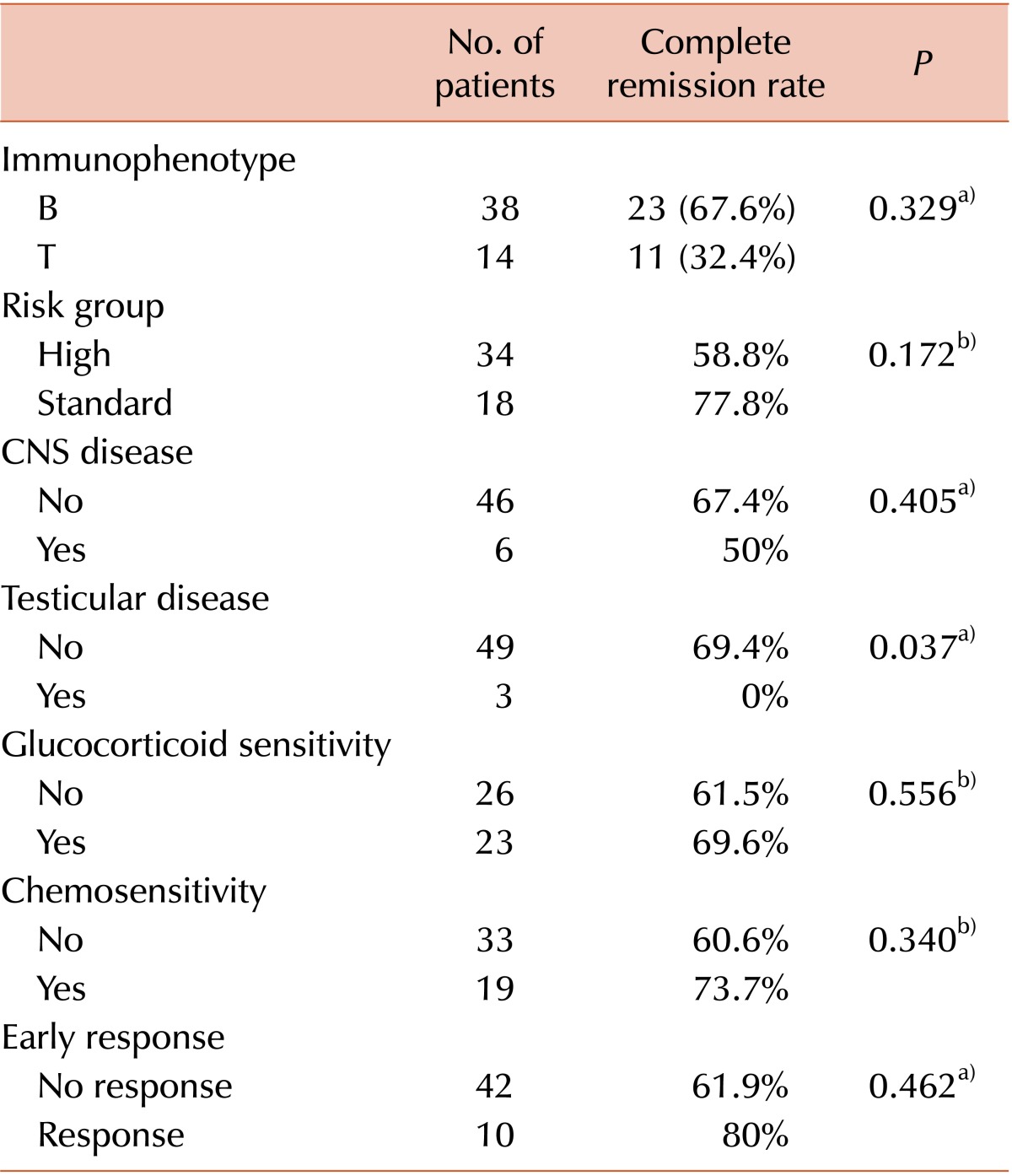
Fifty-two newly diagnosed Philadelphia-negative adult ALL patients with a median age of 34 years (range, 18 to 75 yr) were enrolled in this study. Participants included 35 (67.3%) males and 17 (32.7%) females. Initial WBC counts ranged from 0.5-299×109/L (median, 33×109/L), platelet counts ranged from 5-457×109/L (median, 42×109/L), and hemoglobin levels ranged from 4-14 g/dL (median, 7.6 g/dL). Palpable lymphadenopathy was present in 36/52 patients (69%), 34 patients (65.3%) had splenomegaly, 26 patients (50%) had hepatomegaly, and 21 patients (40.3%) had mediastinal masses. CNS infiltration was found in 6 patients (11.5%). Thirty-eight cases had B-cell ALL while 14 had T-cell ALL. Thirty-four patients (65.6%) were classified as high-risk. Three patients (5.8%) had testicular disease at presentation. GR was encountered in 26/49 patients (53.1%) and 42 patients failed to achieve early response to treatment (80.8%). Thirty-four patients (65.6%) achieved complete remission. Laboratory and clinical findings in relation to the response to induction chemotherapy are shown in Table 2. The event-free survival was 48.1% during the study follow-up period (range, 5 to 40 mo, median, 24 mo).
GR gene polymorphisms
Among ALL patients with the BclI polymorphic variants, 29 (55.8%) had the wild type allele, 20 (38.5%) were heterozygous carriers, and 3 (5.8%) were homozygous for the mutant genotype. The distribution of these genotypes among controls was 66.7%, 30%, and 3.3%, respectively, with no significant difference in distribution between the groups (P=0.608). Among patients with N363S genotype, 49 (94.2%) had the wild type, 3 were heterozygous carriers (5.8%), and none were homozygous for this mutant variant. As for controls, the distribution of these genotypes was 93.3% for the wild type, 6.7% for the heterozygous carriers, and 0% for the homozygous mutant genotype. Regarding the ER22/23EK polymorphism, only 1 patient and 2 control subjects had the heterozygous genotype, while all the other patients and controls had the wild genotype.
The BclI genotypes were not associated with the GC-response (P=0.204); however, such an association could not be examined for the N363S and ER22/23EK genotypes because of the small number of cases with these variant genotypes. Therefore, this association was evaluated after combining the 3 tested genotypes; however, no significant difference was found (P=0.0303) between the wild homozygous allele for the 3 sites (N=26) and any mutant variant (N=23). Furthermore, in accordance with the literature, the patients were sub-grouped into 3 groups: the potentially high GC-sensitivity group (mutant BclI, mutant N363S, and wild ER22/23EK; N=3), the potentially low GC-sensitivity group (wild BclI, wild N363S, and mutant ER22/23EK; N=1), and the other combinations group (N=48). However, there were no significant associations with GC sensitivity (P=0.204).
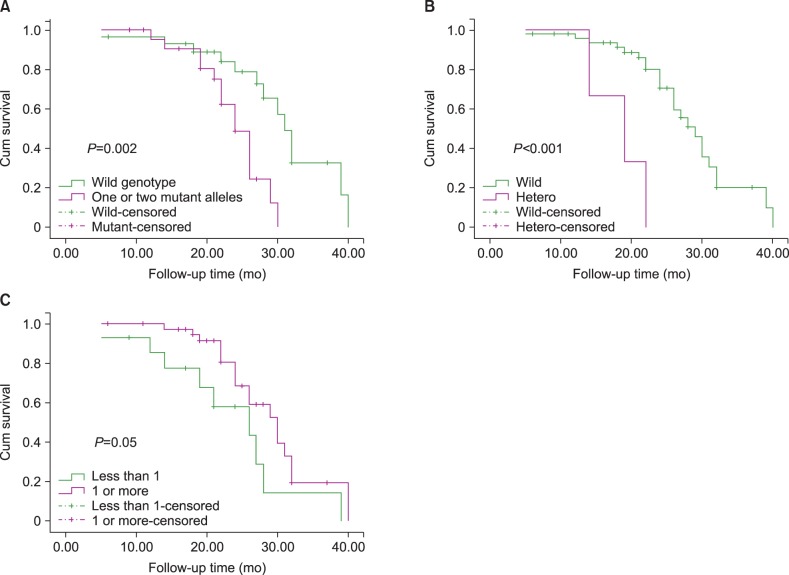
Event-free survival was higher in patients with the wild type BclI allele compared to patients with 1 or 2 mutant alleles (55.2% vs. 39.1%, respectively; P=0.002; Fig. 2A). Regarding the N363S genotype, the event-free survival rate was 51% among wild genotype patients while all 3 patients who had a mutant allele showed an event during the study period (Fig. 2B).
Alpha, beta, and gamma GR isoform mRNA expressions
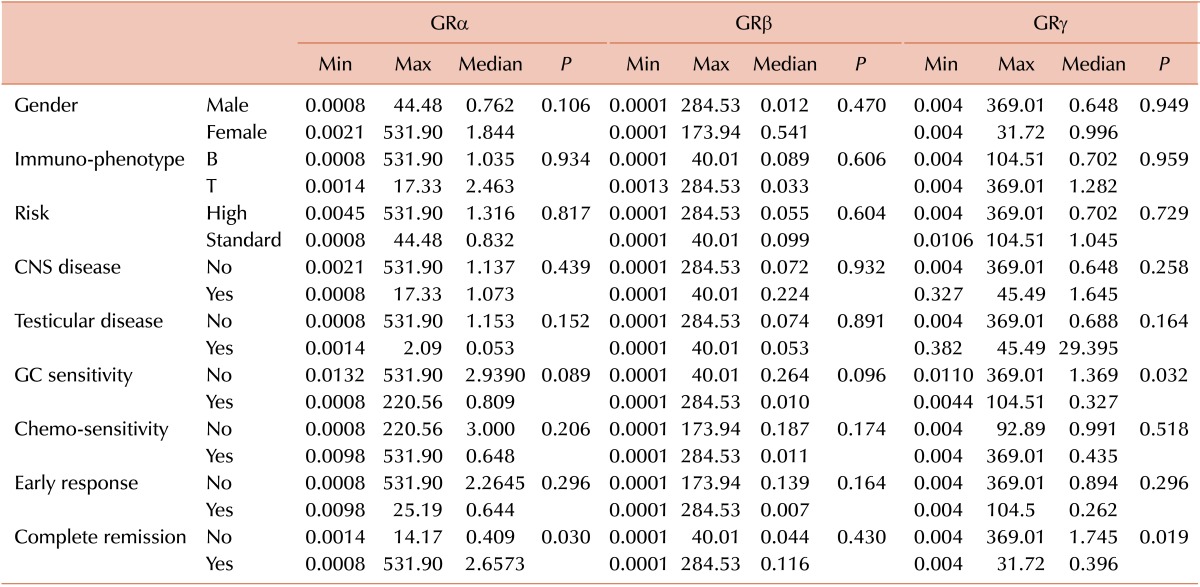
No significant differences were found between ALL patients and normal patients regarding GRα and GRβ mRNA expression; however, GRγ mRNA expression was a bit higher in patients compared to controls (P=0.06). Pretreatment GRα expression was significantly higher in patients who achieved complete remission (P=0.03), but no association was found between the studied laboratory and clinical parameters and GRβ expression. GRγ isoform expression was significantly lower in patients who were GC-sensitive and in patients who achieved complete remission (P=0.032 and P=0.019, respectively, Table 3). On comparing high versus low expression of the 3 isoforms as regards achievement of complete remission, patients with high α or low γ isoform expression were more likely to achieve complete remission (P=0.033 for both) while no significant association was obtained for the β isoform (P=0.559). Patients with an α/β isoform expression ratio equal to or above 1 had an event-free survival of 52.6% while those with a ratio below 1 had an event-free survival of 35.7% (P=0.05; Fig. 2C).
Go to :
DISCUSSION
Interactions among host, disease, and treatment factors determined treatment efficacy in the general ALL model [17]. The effect of GR gene polymorphisms on the efficacy of treatment for childhood ALL has been considered in a few clinical studies but no studies, to the best of our knowledge, have reported results concerning adult ALL patients. The complete remission rate among the studied patients was 65.4%, which is lower than other reports utilizing the same protocol (GRAALL). This could be attributed to sample size issues, delayed diagnoses, or delayed referrals to a hematologist resulting in a stormier and less fruitful remission induction.
The incidence of BclI, N363S, and ER22/23EK polymorphisms reported in the literature varies substantially among different populations. In the present work, the incidence of the BclI, N363S, and ER22/23EK polymorphic alleles among controls was 33.3%, 6.7%, and 6.7% respectively and similar frequencies have been reported by different authors. For example, Fleury et al. observed that among those with the BclI polymorphism in an African population, the GC genotype was 31% [18], while Huizenga et al. reported 6% heterozygosity for the N363S polymorphism and 8.9% for ER22/23EK polymorphisms [19]. In addition, Tissing et al. found the N363S and ER22/23EK polymorphic alleles in 6% and 7.6% of healthy controls, respectively [20].
In the present work, the overall frequency of BclI polymorphic variants (heterozygous and homozygous mutated) was 44.2% in adult ALL patients. However, reports of both lower and higher prevalences of these genotypes are present in the literature. For example, Namazi et al. found that the incidence of BclI polymorphism among 100 pediatric ALL patients was 35%, while Tissing et al. observed that the incidence of BclI polymorphism in a Dutch population was 54.7% [2021]. In agreement with our findings, Wim et al., who studied 57 children with ALL, found no relation between the different GR genotypes and GR or GC resistance [21]. On the other hand, researchers have stated that the ER22/23EK polymorphism is associated with a relative GC resistance [22]. In addition, the N363S and the BclI polymorphisms have been reported to be associated with an enhanced sensitivity to GCs [8]. This may explain the better event-free survival rate among our patients with wild BclI or N363S genotypes
As evidenced by work in transgenic mice with increased and decreased GR expression, the level of GR expression in apoptosis is important [23]. Among the different isoforms of the GR, the α isoform was shown to be responsible for GC-mediated transcriptional activation, while the other isoforms were responsible for disrupting either the hormone binding domain (GRβ) or the DNA binding domain (GRγ) [6]. In the current study, patients who achieved complete remission had higher pretreatment GRα and lower GRγ expression levels. Compared to GC-sensitive patients, the expression of GRγ mRNA was significantly higher in GC-resistant patients. In addition, α isoform expression in excess to β isoform expression was noted in patients with higher event-free survival. Similar results were found by Beger et al. and Haarman et al. [2425]. For example, Beger et al. found that GRγ expression was lower in cells from patients with a good response to GCs compared to patients with a poor response to GCs [24]. Similarly, Gerdes et al. reported that the γ isoform was potentially associated with poor prednisone response in childhood ALL [26]. These data were correlated with cell survival, demonstrating a more pronounced induction of apoptosis in cells from patients with a good response to GCs. This may be linked to the insertion of arginine within the DNA binding domain of the GR that may introduce conformational changes in the 2 zinc fingers thereby reducing DNA affinity [25].
In conclusion, the BclI polymorphic variant of the GR gene was observed more frequently than the N363S and ER22/23EK polymorphisms in Philadelphia-negative adult ALL patients. However, this polymorphism was not associated with the GC response. On the other hand, the wild BclI and N363S genotypes were associated with better event-free survival. In addition, both higher GRα expression and lower GRγ expression were associated with achievement of complete remission, while higher expression of GRγ was associated with GC-resistance. Our data suggest that the level of GR isoform expression may be useful in predicting the GC response, the achievement of complete remission, and event-free survival in adult ALL patients. Further evaluation with a larger cohort is warranted.
Go to :
 XML Download
XML Download