

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
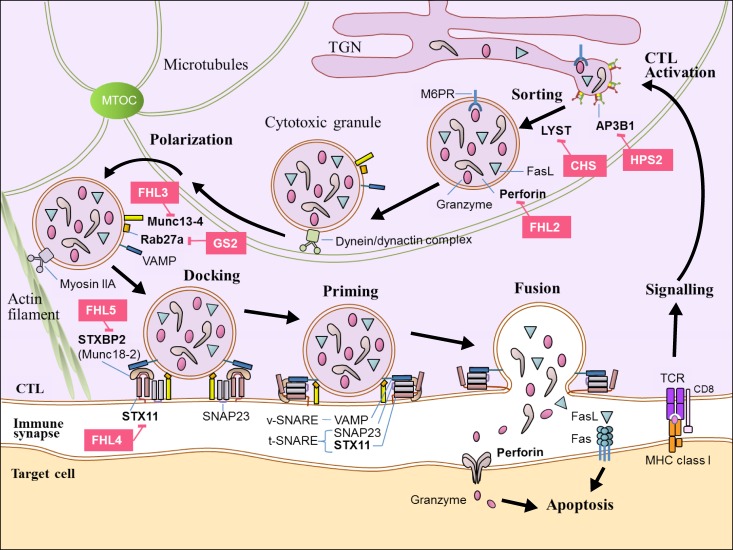
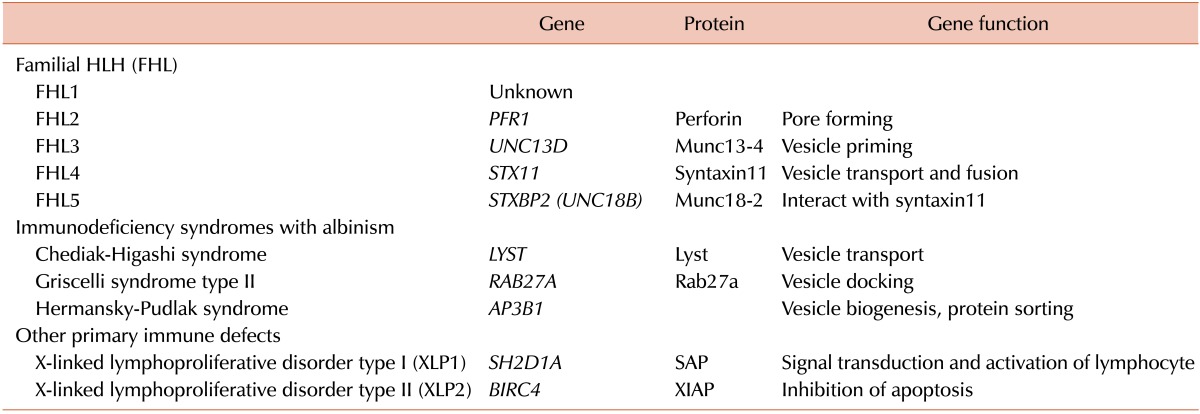
HLH is a life-threatening hyperinflammatory clinical syndrome of uncontrolled immune response which results in hypercytokinemia due to underlying primary or secondary immune defect. HLH can be classified into genetic (primary) and acquired (secondary) forms according to the underlying defect. The primary HLH can be categorized into 2 subgroups, one including 5 subtypes of familial HLH (FHL), and the other expanding subgroup of separate primary immune deficiencies including Chediak-Higashi syndrome (CHS), Griscelli syndrome type 2 (GS2), Hermansky-Pudlak syndrome and X-linked lymphoproliferative (XLP) syndrome 1 and 2 (XLP1, XLP2) [1234567] (Table 1).
A number of genetic defects in transport, processing and function of cytotoxic granules which result in defective granule exocytosis and cytotoxicity of natural killer cells and cytotoxic T lymphocytes have been well identified at the cellular and molecular level [45678910] (Fig. 1). The acquired forms of HLH develop due to a variety of underlying conditions and are more frequent than genetic forms. It is reported that more than 90% of children with HLH were acquired HLH in a nationwide survey in Japan. The most common triggering causes of acquired HLH are infections, autoimmune diseases, and malignancies [45678911].
Important advances have been made during the last 20 years in the diagnosis and treatment of HLH. The Histiocyte Society has proposed diagnostic guideline using both clinical and laboratory findings in HLH-2004 protocol [12], and this has been modified partly in 2009. HLH can be diagnosed by genetic confirmation only with molecular diagnosis consistent with FLH or XLP, or clinically if at least 3 fulfilled out of 4 major symptoms and signs including fever, splenomegaly, cytopenias (at least 2 cell lines), hepatitis, and also at least 1 fulfilled out of 4 laboratory findings including hemophagocytosis, increased ferritin, increased sIL2Rα, absent or very low NK cell function. Hypertriglyceridemia, hypofibrinogenemia, and hyponatremia are also regarded as supportive evidences of HLH diagnosis [13].
The strategies for proper treatment of HLH should include countermeasures for suppression of the hyperinflammation, elimination of triggering causes, killing of infected cells, and replacing defective immune system for patients with genetic disorders. HLH used to be a fatal disease with 1-year overall survival of only 5% [14], but the survival of HLH patients has improved to more than 60% with the use of chemoimmunotherapy combined with HCT over the past 2 decades. However, HCT is still the only curative option of treatment for primary HLH and refractory/relapsed HLH after chemoimmunotherapy. The outcome of HCT for HLH patients has improved steadily during past decades, but HCT for HLH still carries significant mortality and morbidity and there remains controversies in various aspects of HCT [151617181920]. The purpose of this review is to summarize the facts which were proven by previous studies on HCT for HLH and to delineate the future perspectives in the field of HCT for HLH.
HISTORY OF HCT FOR HLH
The first successful allogeneic HCT performed for the treatment of HLH was reported by Fischer et al. in 1986 [21], and the introduction of HCT has dramatically improved the prognosis of the disease thereafter. The Histiocyte Society introduced VP-16 and HCT into the HLH-94 protocol, and these are regarded as the main reasons for the successful improvement in the overall survival around 66±8% of HLH patients who were treated with this protocol. In HLH-94, HCT was recommended for patients with familial, persistent, or recurrent disease, and conventional myeloablative conditioning (MAC) was suggested [22]. Chemoimmunotherapy is only temporarily efficient in the control of FLH, and the outcome is uniformly lethal unless the patient undergoes HCT [1223].
Since 2005, different series of clinical studies have been published on the outcome of HCT for HLH patients reporting 5-year overall survival rates of 50-70% with MAC [182425262728], and 75-92% with reduced intensity conditioning (RIC) [293031]. While the overall survival was increased with HCT using MAC (MAC-HCT), this approach revealed high early transplant-related mortality (TRM) within post-transplant 100 days due to multifactorial causes such as high incidence of veno-occlusive disease (VOD) and pneumonia, and high incidence of primary non-engraftment about 9-22%.
Overall survival rate of the HLH patients not in remission status at the time of HCT was reported to be inferior than that of patients in remission, thus revealing the importance of optimal disease control before HCT [23]. The superior overall survival rate of HCT using RIC (RIC-HCT) regimen for HLH patients compared to MAC were reported by various group since 2006. As the data of RIC-HCT for HLH patients accumulates, various aspects regarding HCT need to be clarified such as indication of HCT, donor selection, timing of HCT, optimal conditioning regimen, and mixed chimerism (MC) after HCT.
INDICATIONS OF HCT
HCT is generally recommended in patients with documented FHL, recurrent or progressive HLH despite recommended chemoimmunotherapy, and CNS involvement [32].
The HLH-2004 protocol recommends HCT for the patients who have genetically verified or familial disease, and for patients with non-familial disease which is severe and persistent or reactivated after 8 weeks of initial therapy. The reactivation of HLH can be diagnosed if the patients have achieved a remission, and then again develop 3 or more of the HLH diagnostic criteria proposed in HLH-2004 protocol.
HCT is mandatory in the treatment of XLP and FHL patients and is the treatment of choice for refractory cases of EBV associated HLH [283334]. HCT should only be performed in patients with GS2 who have a mutation of the RAB27A gene, since only these patients will develop immunodeficiencies and early lymphohistiocytic infiltrates [35].
SELECTION OF DONOR
Selection of optimal stem cell donor and source is important for HLH patients undergoing HCT. It has been reported that the outcome of HCT using matched unrelated donor is comparable to that of HCT using matched sibling donor for HLH patients [181927]. HCT using haploidentical donor for HLH patients who do not have matched donor was reported to be feasible, and the outcome is reported to be improving [3136]. There had been conflicting data regarding the cord blood transplantation (CBT) for HLH.
Japanese group reported comparable outcome of HCT using cord blood stem cells for HLH patients with that of HCT using matched unrelated donor. FHL patients showed either an equal or better outcome even after CBT compared with the recent reports. This study asserted that cord blood might therefore be acceptable as an alternate HCT source for HLH patients, although the optimal conditioning remains to be determined [17]. On the other hand, Korean group reported poorer outcome with CBT [37], and one definite drawback of CBT is that the cases of CBT lack source for donor lymphocyte infusion (DLI) when they show dwindling donor chimerism. Therefore it is necessary for the experts of HLH to consider their institution's experience in HCT when selecting the optimal donor for HCT, as there is considerable center effect.
The possibility of the sibling carrying the disease should be considered when searching for an HCT donor and all family members should be screened for FHL as there are cases with late-onset FHL. To use matched sibling donor for HCT of HLH patients, the donor needs to be confirmed with genetic study and/or NK cell activity test. HLA-matched heterozygous carrier sibling is acceptable as a donor for HCT, and usually these is no relevant dominant negative effect.
TIMING OF HCT
As HCT is indicated in all the patients with primary HLH, it is necessary to start donor search as soon as possible if the diagnosis of primary HLH is made [32]. Rapid identification of genetic immune defects allows differential diagnosis from secondary HLH, thereby enabling early HCT [38].
Patients with active HLH at the time of HCT generally have worse outcomes compared to patients with inactive disease, as active disease increases graft failure and thereby decreases overall survival rate [161827]. Complete responses to conventional HLH therapies are only observed in 50-75% of patients, and the only independent association with improved survival is inactive disease after 2 months of HLH-94 therapy [1939]. Therefore optimal control of disease before HCT is important, and some delay in HCT to treat residual disease optimally is justified. Serial monitoring of soluble CD25 is one of the most useful clinical markers of disease activity in the pre-transplant period, and it can give helpful information for the optimal timing of HCT [23].
However, the best treatment strategy for the reactivated patients before HCT or for patients with residual CNS abnormalities after chemoimmunotherapy is not well established until now, and usually reintensification of treatment before HCT is used to achieve a remission. These subgroup of patients might have the chance of successful HCT, and CNS disease may become permanently controlled after successful HCT [40].
CONDITIONING REGIMEN
Conventional MAC-HCT mostly adopted busulfan, cylophosphamide, etoposide with or without ATG. However, it is repeatedly reported that the outcome of MAC-HCT for HLH patients revealed high early TRM due to multifactorial causes and high incidence of primary non-engraftment around 9-22%. Patients with XIAP deficiency were found to have poor tolerance to MAC [41]. This increased TRM after MAC-HCT has prompted the use of less toxic approach, RIC-HCT. RIC-HCT has been most extensively studied in patients with nonmalignant disorders and sufficient data now exist for HLH to support its routine use even in patients without comorbidity. The goals of a RIC regimen are to prevent graft rejection and to establish stable donor-derived hematopoiesis at a level sufficient for cure of the underlying disease. RIC regimens have also enabled HCT to be performed in children with preexisting comorbidities that preclude conventional conditioning [42].
RIC with alemtuzumab, fludarabine, and melphalan has demonstrated better outcomes in HCT, and its use is increasing [2943]. Fludarabine-based conditioning regimen including melphalan and alemtuzumab or ATG is one of the widely used RIC regimens for HLH patients, and various modifications of this combination were reported. Marsh et al. reported a 3-year survival rate of 92% in their RIC cohort, compared with 43% in their MAC cohort. However, high incidences of MC and graft loss are significant concerns after RIC-HCT. The transplant physicians treating HLH should be well aware of the countermeasures in these circumstances [43].
Alemtuzumab is a humanized recombinant monoclonal antibody directed against CD52 on lymphocytes, and it targets both activated T cell and macrophages. It is frequently included in RIC regimens as it is an effective immunosuppressant. Alemtuzumab persists at lympholytic concentration for 1-2 months after infusion, and it can exert effects on both the recipient and the graft due to this long pharmacologic half-life. Administration of alemtuzumab distal to the stem cell infusion date (beginning about day -21), likely produces predominant effects on the recipient, with decreased risk of graft rejection but less effect on graft-versus-host disease (GVHD) prevention. Proximal administration (beginning about day -9) may result in more circulating drug after stem cell infusion and in vivo T-cell depletion of the graft, thereby resulting in reduction of GVHD, increased risk of graft failure, and impaired immune reconstitution. Intermediate administration (beginning day -13) may balance these risks and benefits. Cincinnati group recently reported that intermediate RIC reduces the risk of MC, is associated with a low incidence of acute GVHD, and decreases the need for additional hematopoietic cell products after HCT [434445]. Although the RIC approach appears promising, more follow-up in larger cohort of HLH patients undergoing HCT is needed to ascertain the long-term outcome [5].
Conditioning regimens with reduced toxicity based on melphalan or treosulfan are promising alternatives. It is reported that fludarabine, treosulfan, alemtuzumab, and thiotepa represent a conditioning regimen with a high rate of disease-free survival and low toxicity in the high risk group of patients with hereditary HLH [46]. RIC-HCT using a haploidentical donor was reported to sufficiently restore immune regulation in infants with FHL, while decreasing TRM and long-term sequelae [47]. Japanese group reported the feasibility of RIC in unrelated CBT for patients with primary HLH using melphalan, fludarabine and anti-lymphocyte globulin or anti-thymocyte globulin [4849]. Choice of conditioning regimen when CBT is the only option should be carefully considered, as the lack of source of DLI is a significant concern due to the high incidence of MC after RIC-HCT [43].
GRAFT FAILURE AND TRM
MAC-HCT using busulfan, cyclophosphamide, and etoposide with or without ATG has long been the standard of care for patients with HLH. However, MAC-HCT is associated with high TRM (30-50%), and main causes of early TRM include infections, VOD, pneumonitis, graft failure, and GVHD [121824252627282950].
As TRM may be due to the incomplete control of HLH before HCT in some patients, every effort must be made to achieve remission of underlying FHL before HCT. However, significant TRM has also been noted in patients with apparently good control of underlying FHL before HCT. It is possible that occult liver or lung damage from HLH may predispose FHL patients to high rates of VOD or pneumonitis when treated with a busulfan-based MAC. A significant number of early deaths before post-transplant 100 days are attributed to HLH reactivation. The patients who survived 100 days after HCT with durable engraftment usually experience long-term disease free survival [1723253051]. Most deaths occur in the first year post-transplantation, and the likelihood of relapse is limited after the second year [2032].
MIXED CHIMERISM (MC)
Approximately half of patients with HLH treated with RIC, however, experience MC, which may be unstable in the early post-transplant months, and raises concerns for subsequent HLH relapse and graft loss. This may be due to the inclusion of alemtuzumab in the preparative regimen, as a significant effect of timing of alemtuzumab was noted upon the incidence of MC. Rapid immunosuppression withdrawal, donor lymphocyte infusion (DLI), or stem cell boost are frequently employed interventions to prevent MC progression, graft loss, and need for second transplant. However further study in larger cohort of patients are needed to establish consensus approach in the optimal dosing, timing, and efficacy of these interventions [435152].
Murine studies and clinical observations suggested that a stable chimerism with 10-20% donor cells may be sufficient for correction of the underlying condition in a variety of non-malignant conditions. Mixed hematopoietic or T-cell chimerism above a minimal threshold restores perforin-dependent immune regulation in perforin-deficient mice [453]. It appears that whole blood donor chimerism above 10-20% does indeed act against HLH, as HLH relapse was noted only after donor chimerism fell to less than 10%. Frequent monitoring of chimerism studies is essential, and centers should be prepared to stabilize donor chimerism with early withdrawal of GVHD prophylaxis or administration of DLI if needed [43].
The timing of alemtuzumab administration is closely linked to underlying disease, thereby making it difficult to draw definitive conclusions regarding the influence of timing on development of MC and graft loss. Distal administration of alemtuzumab in patients with non-malignant diseases resulted in a low incidence of MC and graft loss supporting this dosing strategy in this subset [445254].
Decisions regarding DLI should currently be based on patient chimerism trends, availability of DLI product, active infections, history of GVHD, and other factors. DLI is often recommended when donor contribution to MC is rapidly or persistently declining during the early post-HCT period towards thresholds that cause concern for eventual HLH relapse and graft loss. The patients with trends of decreasing donor contribution to hematopoiesis to levels lower than 40-60% within the first 6 months post-transplant need to be considered for DLI at this point so as not to further decrease to levels below 20%. As patients with earlier onset or more rapid decline of donor chimerism appear to be at higher risk of graft loss or HLH recurrence, the onset and rate of decline of donor chimerism are also to be considered [45].
OUTCOME AND PROGNOSIS OF HCT FOR HLH
The overall estimated 3-year survival who received HCT according to HLH-94 protocol was 64%. The best results following MAC have been achieved when HLA-matched related or unrelated donors were used, and CNS disease was absent or quiescent at the time of HCT. The best results with HCT have been observed in children who achieved prompt and complete response to chemoimmunotherapy prior to HCT. Thus the disease state after initial treatment, the stem cell source of the transplant, and the donor type were the important prognostic factors that affected the overall survival of the HLH patients who underwent HCT [272829303151].
It is also reported in a multivariate analysis that a younger age at diagnosis, severe transaminasemia, and a coagulation abnormality were also other independent prognostic factors for survival [55]. Ohga et al. reported that EBV-HLH patients showed a better prognosis after HCT than FHL patients in their series of patients [1733]. Children with HLH may have long-term significant cognitive and psychosocial impairments, even after a successful HCT. These impairments can occur despite no obvious neurologic involvement with the disease process at diagnosis [56]
HLH AFTER HCT (HCT-HLH)
HCT-HLH is thought to develop more often than previously suspected, because the number of HLA-mismatched HCT is currently increasing. A prospective observational study on HCT-HLH with 171 patients who underwent HCT reported a relatively high incidence (8.8%) after allogeneic HCT [57].
Because it is difficult to use immunosuppressive or cytoreductive agents in the immune-compromised stage within the first 30 days after HCT, the criteria for HCT-HLH in the early-onset group need to be stringent. In patients who develop a sustained fever without an apparent causative infection in early post-transplant period, HCT-HLH should be included in the differential diagnosis. Very high levels of serum ferritin, soluble IL-2 receptor, and the presence of hemophagocytosis are findings suggestive of HLH. HLH directed therapy should be considered for these patients, and early treatment with low-dose VP-16 appears to be a successful approach for early-onset HCT-HLH. [5859]
SPECIAL CONSIDERATIONS IN SPECIFIC SUBSETS OF HLH
HCT for FHL5
Mutations in STXBP2 affect not only cytotoxic T lymphocytes but also cause changes in the intestinal and renal epithelium resulting in severe, osmotic diarrhea and renal proximal tubular dysfunction. A severe, life-threatening form of enteropathy may precede the typical features of FHL, and FHL5 must also be considered as a differential diagnosis in patients with intractable diarrhea. As these defects persist after successful treatment of HLH by HCT, FHL5 patients who received otherwise successful HCT in their childhood may suffer from gastrointestinal, nephrological, neurological and other non-hematological disorders. Clinical manifestations in FHL5 patients despite successful HCT may therefore be related to defective membrane trafficking in the gut and kidney [60].
HCT for CHS, GS2, and XLP
CHS, GS2, and XLP are diseases showing similar immunological manifestations, and predispose to a fulminant HLH. Treatment delay increases the risk of fatal outcome and may increase the risk for neurological complications. HLH treatment can be an effective first line treatment to induce remission in patients with CHS, GS2, and XLP [61].
HCT for CHS
The most effective treatment for the hematologic and immune defects in patients with CHS is HCT, despite no evidence of efficacy in delaying or preventing progressive neurologic dysfunction. Although comparative trials are lacking, RIC may be better than MAC with regard to toxicity and overall survival. A prompt diagnosis of the early-onset form of CHS, with special emphasis on the molecular characterization and analysis of CTL cytotoxicity, might help identify patients with a high risk of developing HLH. Patients with absent CTL cytotoxicity might need early HCT because of their high risk of developing HLH. Normal CTL cytotoxicity or bi-allelic missense mutations do not exclude the development of HLH, but a more conservative approach is justified [62].
HCT for GS2
HCT is an efficient treatment for curing the immune disorder of GS2. Patients with GS2 should urgently be treated with HCT after diagnosis for the risk of HLH. Neurologic HLH before HCT is a major concern, and the neurologic sequelae after otherwise successful HCT are not uncommon. Considering the high observed toxicity of HCT in GS2, RIC might be recommended. Improvement of the transplantation procedure is needed to reduce its toxic effects, and diagnosis should be made as early as possible to reduce long-term, post-transplant neurologic sequelae [6364].
HCT for XLP1
XLP1 is a rare immunodeficiency characterized by severe immune dysregulation and caused by mutations in the SH2D1A/SAP gene. Clinical manifestations are varied including HLH, lymphoma and dysgammaglobulinemia, often triggered by Epstein-Barr virus infection. HLH still remains the most severe feature of XLP1, and HCT should be undertaken in all patients with HLH as the outcome without transplant is extremely poor. The outcome of HCT for other manifestations of XLP1 is very good, and patients must be monitored closely for evidence of disease progression if HCT is not undertaken [65].
Marsh et al. reported that RIC consisting of alemtuzumab, fludarabine, and melphalan is a feasible approach for patients with XLP1, and showed good outcomes in most patients with no relapses of HLH or lymphoma observed in their series. RIC should especially be considered for patients with XLP1 who have a history of HLH [66].
HCT for XIAP (X-linked inactivator of apoptosis) deficiency (XLP2)
Patients with XLP2 were found to have poor tolerance to MAC, and the value of HCT in XIAP deficiency is an ongoing matter of debate. It is reported that conditioning regimen and HLH activity affected outcome, and the survival after RIC-HCT of patients in remission from HLH was 86%. In this report, the survival after MAC was quite poor, and the authors concluded that MAC should not be used for patients with XIAP deficiency. RIC regimens should be pursued with caution and, if possible, efforts should be made to achieve HLH remission before HCT in these patients [41]. However, the good long-term outcome in several patients who didn't receive HCT, a confirmed low risk of lymphoma development, and the reported high complication rate of HCT in this disease certainly warrants general caution with HCT. [416768].
HCT for CNS-involved HLH
It was reported that very young HLH patients who are at high risk of fatal FHL with persistently deficient NK activity and/or overt CNS disease require appropriate HCT to reverse CNS disease and achieve a complete cure. Most of the HLH patients with CNS involvement surviving HCT show improvement in neurologic function and cognitive development, and long-term follow-up reveal a normal or near-normal quality of life in most of them. These results strongly indicate the efficacy of HCT for primary HLH patients with CNS disease. Late complications of prior CNS damage can manifest months to years after HCT with neurocognitive deficits [13326970]. It is also reported that notable response to the therapy with reduction of the CNS lesions and normalization of the brain metabolite detected by MR spectroscopy could be observed after successful HCT [71].
CONCLUSION AND FUTURE PERSPECTIVES
As there have been considerable accumulations of data with regard to the various uncertain issues and controversies in HCT for HLH, it is more and more expected that the outcome of HCT for these patients might be significantly improved in in near future.
With the increased use of whole genome sequencing approaches, it is expected that the genetic and molecular bases of the remaining unknown familial cases of hereditary HLH will soon be elucidated [6].
Novel treatment modalities, such as gene therapy for correction of perforin defects, are currently under evaluation. Preliminary data on perforin gene transfer into hematopoietic stem cells of a mouse model of perforin-deficiency have shown encouraging results of improving immune dysregulation [7273].
Together with the improvements in the HCT for patients with HLH, ongoing efforts to improve the pre-transplant treatment of HLH will also improve the outcome of HCT. More data through clinical trials of salvage therapies and second-line treatment are needed to improve HCT outcomes.
 XML Download
XML Download