

 PDF
PDF ePub
ePub Citation
Citation Print
Print


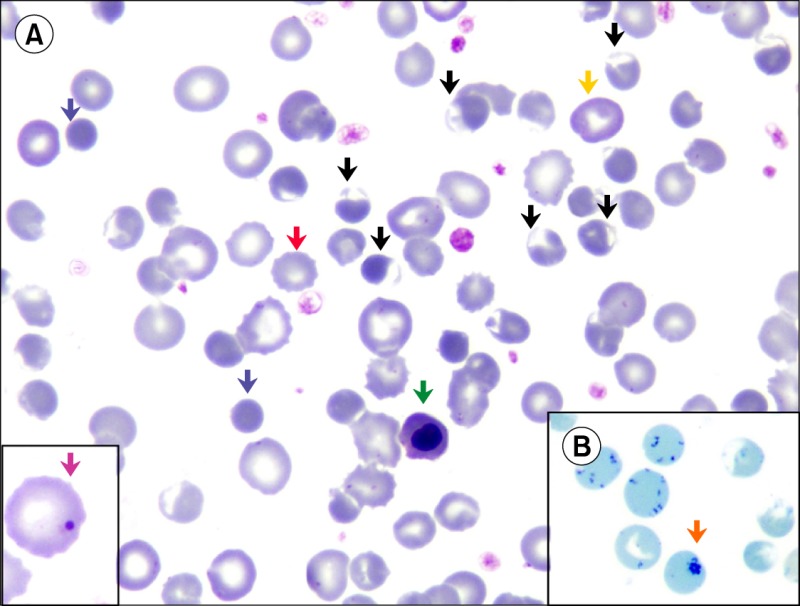
A 65-year-old man presented with a 5-day history of fever. He took an antimalarial drug (Fansidar;sulfadoxine/pyrimethamine) without being tested for malarial parasite. After 2 days, he developed dyspnea. Examination revealed pallor. Complete blood count showed the following: hemoglobin (Hb), 7.4 g/dL; hematocrit, 23%; mean corpuscular volume, 105 fL; mean corpuscular Hb, 34 pg; white blood cell, 28.1×109/L with 81% neutrophils; platelets, 217×109/L; and corrected reticulocyte count, 20%. Peripheral blood smear (PBS) displayed numerous blister cells (black arrow) and other hemolytic features such as spherocytes (blue arrow), polychromasia (yellow arrow), nucleated red blood cell (green arrow), and Howell-Jolly body (A, pink arrow). Reticulocyte preparation revealed Heinz bodies (B, orange arrow). Acanthocytes (red arrow) signifies acute renal injury. Further workup showed the following: total bilirubin, 3.2 mg/dL (reference range, 0.1-1.2); indirect bilirubin, 2.2 mg/dL (0.1-0.8); serum haptoglobin, <0.01 g/L (0.3-2); serum creatinine, 2.6 mg/dL (0.8-1.3); and glucose-6-phosphate dehydrogenase (G6PD) level, 5.1 U/gHb (6.7-14.3). G6PD level measured after 8 weeks was 0.2 U/gHb He had no similar episode in the past. Urinary pseudomonas isolates was the likely cause of the fever. According to the PBS findings and low G6PD levels, we made a diagnosis of G6PD deficiency, which is an X-linked hereditary disease characterized by low levels of G6PD, a metabolic enzyme involved in the pentose phosphate pathway. Antimalarials usually induce acute hemolysis in G6PD-deficient individuals. Late presentation is not uncommon, where peripheral smear can be useful in diagnosis without medical or family history.
 XML Download
XML Download