

 PDF
PDF ePub
ePub Citation
Citation Print
Print


TO THE EDITOR: Granulocytic sarcoma (GS) or myeloid sarcoma (MS) is an extramedullary tumor comprising myeloblasts or immature myeloid cells. This type of tumor commonly occurs in subperiosteal bone structures of the skull, paranasal sinuses, as well as the sternum, ribs, vertebrae, pelvis, lymph nodes, and skin [1]. GS is frequently mistaken for non-Hodgkin lymphoma (NHL), small round cell tumors (neuroblastoma, rhabdomyosarcoma, Ewing's sarcoma/primitive neuroectodermal tumor, and medulloblastoma), or undifferentiated carcinoma. The diagnosis is overlooked in about 50% of the cases when immunohistochemistry (IHC) analysis is not performed [2]. The most common diagnosis, suggested in these situations, is NHL [3]. MS may be the first manifestation of AML, preceding it by months or years, or represent the initial manifestation of relapse in previously treated AML in the remission stage [4]. Isolated MS, defined by the absence of a history of leukemia, myelodysplastic syndrome (MDS), or myeloproliferative neoplasm along with a negative bone morrow biopsy has been described in only a few case reports [5].
Here we report a case of a small gut mass that presented with features of intestinal obstruction necessitating exploratory laparotomy and resection anastomosis of a segment of the small gut. The mass was evaluated for lineage differentiation by IHC and the results correlated with clinicopathologic findings as well as cytogenetic and molecular studies.
CASE
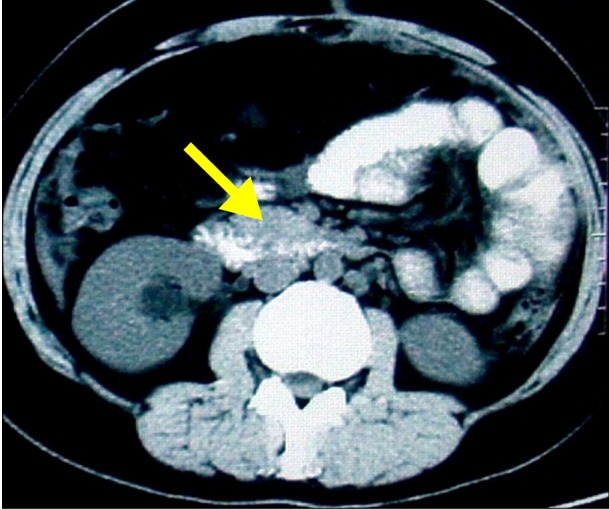
A 27-year-old woman presented with recurrent, colicky abdominal pain associated with occasional vomiting for 2 months. There was no history of fever, jaundice, hematemesis, or melena. She had been hospitalized several times and treated conservatively. The patient was conscious, alert, oriented, and afebrile, and her vitals were within normal limits. No pallor, edema, jaundice, clubbing, or superficial lymph node enlargement were present. Her abdomen was soft, non-tender, and not distended. Other systemic examinations revealed no abnormality. Contrast enhanced computerized tomography of the abdomen showed a soft tissue mass lesion (Fig. 1) in the left side of the mesentery with adherent small gut loops.
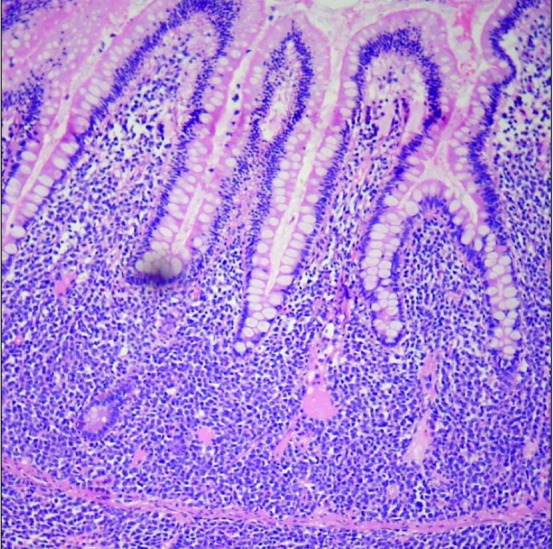
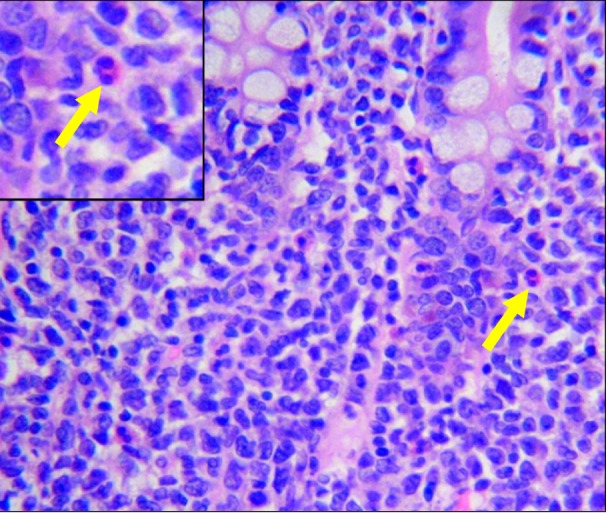
Exploratory laparotomy was performed. There was moderate ascites without liver nodules or peritoneal deposits. There was an 8.0×7.0 cm globular mass with serosal involvement in the ileum, located 40 cm proximal to the ileo-cecal junction causing luminal obstruction and proximal dilatation, with no apparent mucosal involvement and thickening of the adjacent small bowel. The involved Ileal segment was resected with a 10 cm proximal and a 5 cm distal margin, and a side-to-side ileo-ileal anastomosis was performed. On gross examination of the specimen, there was a tumor, 6 cm in diameter, extending outwards into the mesentery and protruding into the intestinal lumen. The cut surface was grayish and fleshy. A total of 10 tiny lymph nodes were seen in the mesentery. Microscopically, the small intestine showed a tumor composed of sheets of atypical large cells with moderate to scanty cytoplasm, a high nucleo-cytoplasmic ratio, and occasional prominent nucleoli. A fair number of eosinophils were also observed (Fig. 2, 3). The tumor cells infiltrated the muscle coat of the intestine and extended up to the serosa. A morphological diagnosis of high grade NHL, large cell type vs. granulocytic sarcoma were differential diagnoses. The surgical resection margins or the lymph nodes were not involved. On IHC analysis, the tumor cells were positive for the leukocyte common antigen, CD117, CD34, myeloperoxidase (MPO), and CD43 and negative for CD20, CD3, CD5, CD10, and CD23. Thus, a final diagnosis of GS (MS) of the small gut was made. A peripheral blood smear showed apparently normal WBC counts with normal differential and platelet counts. Bone marrow aspiration showed normocellular marrow with tri-lineage differentiation. Blast counts were not increased. Conventional cytogenetics showed a normal 46, XX chromosomal pattern. Subsequently, the marrow material was assessed for the presence of common translocations by multiplex RT-PCR and inv(16)(p13;q22); CBFB-MYH11 was detected.
In this case, the bone marrow did not show any morphological involvement; however, the detection of the molecular marker of inv(16)(p13;q22) fulfills the criteria of AML diagnosis as defined by the World Health Organization in 2008 [1]. Routine biochemical parameters including serum potassium, calcium, phosphorus, and magnesium were within the reference ranges. Viral markers were negative. After proper counseling, the patient was treated with standard "3+7" daunomycin and cytarabine as remission induction followed by 3 cycles of consolidation therapy with high dose cytarabine [6]. The clinical course of the patient was uneventful during chemotherapy except for 2 occasions of febrile neutropenia, which were managed successfully by antimicrobials. Post consolidation, inv(16)(p13;q22) was negative from bone marrow. Post chemotherapy, she is on regular follow up and doing well.
DISCUSSION
In the absence of a clinical history of leukemia, a diagnosis of MS can be difficult, despite efforts to establish a tissue diagnosis. MS can often be misdiagnosed, most typically as NHL, in up to 46% of patients [7]. Primary MS has been described in virtually every anatomic location, with a particular predilection for the skin, soft tissue, bone, periosteum, and lymph nodes. Gastrointestinal involvement is infrequent [8]. Acute abdominal pain resulting from partial or complete bowel obstruction is the most common clinical presentation. Grossly, the lesions present as polypoid or exophytic masses, regions of wall thickening and/or ulcerations with a high proclivity for mesenteric and peritoneal dissemination [9]. The present patient had a globular mass with serosal involvement in the ileum, located 40 cm proximal to the ileo-cecal junction causing luminal obstruction and proximal dilatation.
Similar to patients with a history of leukemia, the tissue samples should be sent for IHC, flow cytometry, fluorescence in situ hybridization, cytogenetic and molecular analyses. In addition, once the extramedullary mass has been established, bone marrow aspiration and/or biopsy samples should be subjected to similar analyses [6]. IHC is the most practical method for establishing the diagnosis of MS and can be easier than flow cytometry, which requires cells to be in suspension. IHC can also discriminate between myeloid and non-myeloid cells by using monoclonal antibodies against MPO and lysozyme. MPO staining is very often positive with malignant cells of extramedullary tumors, which is a quick way of establishing the diagnosis and ruling out other tumors [10]. Primary GS of the small intestine is an uncommon entity with a unique histopathology mimicking other solid neoplasms, making it a diagnostic challenge [11]. Although the optimal timing and the treatment of isolated MS are not clear, delayed or inadequately systemically treated isolated MS will almost always progress to AML [12]. The time to the development of AML in this setting ranges 5-12 months [13]. Using RT-PCR, gene fusions specific for AML in the bone marrow of patients with isolated MS have been detected, suggesting that marrow involvement might occur early in the process before clinical detection [14]. Very rarely, cases of MS originating from blasts with inv(16) have also been reported, predominantly occurring with intestinal manifestations [15]. According to Bakst et al. [6], after the standard course of remission-induction chemotherapy, similar to that used for AML, each patient should be evaluated individually and assessed according to multiple prognostic factors including age, comorbidities, degree of dissemination, and cytogenetic/molecular abnormalities, when deciding on a post-remission strategy. Moreover, there is no evidence that an approach combining chemotherapy with radiotherapy is superior to aggressive chemotherapy alone. Patients with MS have a predisposition to extramedullary relapses. After treatment, patients with MS are followed up similarly to other AML patients and undergo detailed physical examinations and routine peripheral blood analyses to confirm continued complete remission.
In summary, the present findings suggest that a high index of suspicion is required to prevent misdiagnosis of MS, and sometimes, molecular analysis is essential for decision making especially when the results for conventional cytogenetics are inconclusive.
 XML Download
XML Download