

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hereditary hemorrhagic telangiectasia (HHT), also known as Osler-Weber-Rendu syndrome, is an autosomal dominant inherited vascular dysplasia characterized by mucocutaneous telangiectasias and visceral arteriovenous malformations [1, 2]. Patients with HHT experience repeated epistaxis and gastrointestinal bleeding with severe iron-deficiency anemia [1], and the organs that are usually affected are the lungs, liver, and brain [1]. The abnormal vessels of HHT are vulnerable to bleeding because of their inadequate vessel wall structure and high perfusion pressure [3]. The cellular mechanisms underlying the generation of HHT telangiectasia and arteriovenous malformations have been unraveled, with recent reports focusing on a defective response to angiogenic stimuli in various settings [2]. Serum concentrations of transforming growth factor beta (TGF-β), activin receptor-like kinase 1, and vascular endothelial growth factor (VEGF) are significantly higher in patients with HHT [3, 4]. TGF-β stimulates the production of VEGF, which plays a key role in angiogenesis [4]. Generally, a conventional dose (5-10 mg/kg) of bevacizumab is administered intravenously as a direct anti-angiogenesis strategy to treat patients with severe HHT, but the relative efficacy of lower-dose intravenous bevacizumab is not well known. We report a substantial effect of low-dose bevacizumab (2 mg/kg) in a patient with severe anemia due to HHT.
Go to : 
CASE REPORT
A 55-year-old man presented with long-standing epistaxis, recent melena, and dizziness. He had a three-generation family history of chronic epistaxis, anemia, and regular blood transfusions for 16 years (Fig. 1). Physical examinations showed mucocutaneous telangiectasias of the lips, tongue, finger tips, and lower eyelids (Fig. 2A), along with finger clubbing and pale conjunctivae. Initial laboratory findings were 6.0 g/dL hemoglobin (90 fL MCV, 27 pg MCH), 308×109/L platelets, 15.4% red blood cell distribution width, 6.4% reticulocytes, 25 µg/dL serum iron, and 13.17 ng/mL serum ferritin. Endoscopic gastroduodenoscopy (EGD) and colonoscopy were performed for the anemia workup, during which numerous telangiectasia of the total gastric mucosa with old blood clots and easy touch bleeding were observed (Fig. 2B). We treated the patient using an argon plasma coagulator (APC) (Fig. 2B), which successfully stopped the melena. During the hospitalization period, total 8 units of red blood cell were transfused. However, he was readmitted 1 month after discharge with dizziness and anemia because of repeated gastrointestinal bleeding. Repeated endoscopic treatment with APC of multiple gastric telangiectasias was performed. Concurrently, other bleeding foci were screened using a red blood cell nuclear scan, and radioactivity was detected in the stomach, jejunum, ileum, and upper small bowel areas on both dynamic and 24-h delayed images. We needed another 8 units of red blood cell transfusion to raise hemoglobin level. As treatment methods with oral iron and endoscopic APC both failed to raise hemoglobin levels, we considered using the anti-VEGF antibody, bevacizumab. The patient first refused bevacizumab treatment due to financial problems. It was only after several failures to control local bleeding with endoscopic APC that he finally agreed to the bevacizumab treatment. Standard regimens for HHT treatment using bevacizumab have not been established, and the minimum intravenous bevacizumab dosage is >5 mg/kg in almost all reported cases. We decided to administer low-dose intravenous bevacizumab (2 mg/kg) considering his financial status. The patient received four courses of intravenous bevacizumab, 2 mg/kg per course, every 3 weeks. Despite the low bevacizumab dosage, both hemoglobin and serum ferritin levels increased and maintained higher levels after treatment, and the frequency of red blood cell transfusions decreased beginning at the early phase of treatment (Fig. 3). He had been transfused with more than four units of packed red blood cells every 2 weeks before the bevacizumab treatment. After the low-dose intravascular bevacizumab administration, he did not need blood transfusions for 2 months. Follow-up EGD also demonstrated improvement in the numerous telangiectasias of the gastric mucosa (Fig. 2C). However, blood transfusions resumed after the fourth course of bevacizumab treatment. Nevertheless, the frequency of blood transfusions was reduced by half (every month), and epistaxis frequency per month decreased by 50% (Fig. 3). The patient could not continue treatment because of his financial status.
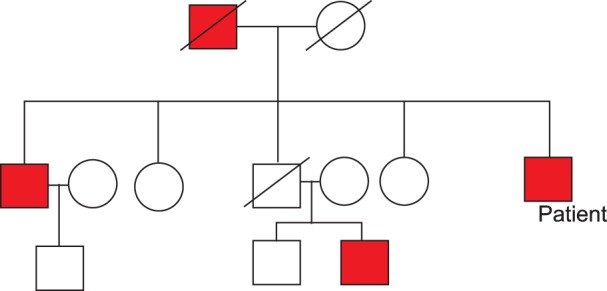 | Fig. 1Pedigree of the patient's family. Red box indicates those affected by hereditary hemorrhagic telangiectasia.
|
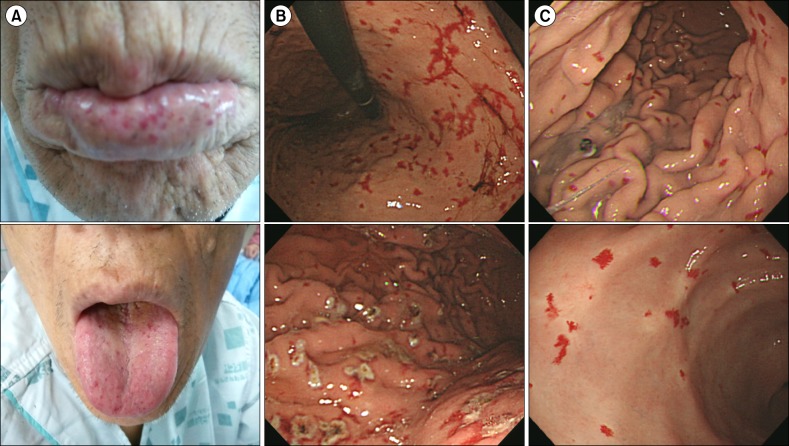 | Fig. 2(A) The lips and tongue showed mucocutaneous telangiectasias. (B) Numerous telangiectasia lesions of the total gastric mucosa with old blood clots and easy touch bleeding patterns were observed by endoscopic gastroduodenoscopy (EGD). Argon plasma coagulation (APC) provided successful management. (C) Follow-up EGD showed improved telangiectasia of the gastric mucosa after bevacizumab therapy.
|
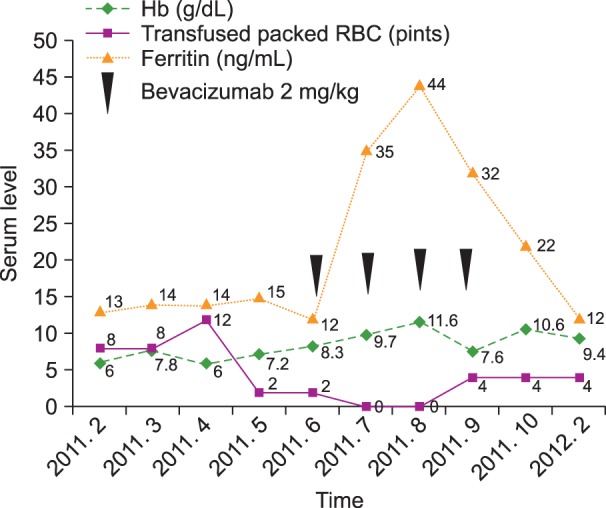 | Fig. 3Hemoglobin and serum ferritin levels increased after administration of low-dose intravenous bevacizumab and were maintained. The frequency of red blood cell transfusions decreased. However, the hemoglobin level again decreased, and blood transfusions were required after the fourth bevacizumab cycle.
|
Go to :
DISCUSSION
HHT is a familial disorder characterized by delicate, ecstatic vessels in the skin, mucous membranes, and viscera [5]. HHT is an autosomal dominant inherited disorder, in which small telangiectasias on the face represent an important cosmetic problem, and larger lesions lead to iron deficiency anemia due to chronic blood loss [6]. Early diagnosis of HHT is important to avoid complications from arteriovenous malformations, and proper clinical management of symptomatic as well as pre-symptomatic individuals is necessary [7]. Several studies that aimed to guide management practice have been published recently [2]. New data suggest surgery and cauterization for nosebleeds as a local bleeding control method [2]. Patients with HHT and gastrointestinal bleeding require numerous endoscopic examinations or surgical resections to prevent recurrent bleeding [8]. In addition, the number of required blood transfusions can be reduced by hormonal treatment (estrogen/progesterone preparations or danacrine) in patients with HHT and gastrointestinal bleeding [8]. However, this therapy is of limited applicability, particularly for male patients, as they often suffer from pronounced side effects such as gynecomastia, edema, and feminization [8].
Bevacizumab is a full-length recombinant humanized antibody active against all VEGF-A isoforms, which plays differing and non-overlapping roles in the induction and patterning of angiogenesis [9]. Bevacizumab is an anti-neoplastic agent and is commonly used to treat various cancers, including colorectal, lung, breast, and kidney cancers, as well as glioblastomas [9, 10, 11]. Common adverse effects of intravenous bevacizumab include bleeding or hemorrhage, hypertension, proteinuria, gastrointestinal symptoms such as abdominal pain or vomiting, and venous or arterial thromboembolic events [10]. According to the 2009 HHT guidelines, intravenous bevacizumab is another treatment option for patients with HHT [2]. Several reports of successful HHT treatment with intravenous bevacizumab have been published in Western countries [12]. However, the standard dosage of intravenous anti-VEGF regimens for severe HHT treatment has not been reported. In particular, the conventional (5-10 mg/kg) dose of intravenous bevacizumab that has been reported so far has not been applied to patients with gastrointestinal bleeding. In previous reports, at least 5 mg/kg intravenous bevacizumab was administered for initial and maintenance treatment [6, 13, 14].
Our patient had received countless blood transfusions due to recurrent anemia until June 2011. Although low-dose intravenous bevacizumab (2 mg/kg) was administered due to the patient's financial status, it reduced the frequency of blood transfusions required, even during the early phase of treatment. The patient had never experienced a period longer than 2 weeks without receiving a blood transfusion in the 16 years before bevacizumab administration, but he did not require a blood transfusion for 2 months after the bevacizumab therapy. Furthermore, he did not complain of any adverse effects during the bevacizumab treatment. However, his hemoglobin level began to decrease after the fourth course of bevacizumab treatment, and blood transfusions resumed. A relapse in epistaxis or mucocutaneous bleeding after bevacizumab treatment was reported by Bose et al. [4], likely due to the short half-life of bevacizumab (20 days) [11] with spontaneous regeneration of VEGF in its absence [3, 12]. Our results demonstrate that low-dose intravenous bevacizumab (2 mg/kg) was inadequate to maintain stable hemoglobin levels due to severe gastrointestinal bleeding in the long term. However, an early clinical effect was confirmed in our case. A few cases of treatment with low-dose (2-3 mg/kg) intravenous bevacizumab for severe epistaxis have been reported as initial treatments of <6 months' duration, but long-term data are lacking [15].
In our case, the commonly encountered skin and other side effects of a conventional dose of intravenous bevacizumab were minimal and tolerable. Low-dose intravenous bevacizumab was effective at the beginning of treatment. However, we could not find the optimal duration of the treatment because the present patient discontinued the treatment. This case suggests that the use of low dose (2-3 mg/kg) of intravenous bevacizumab can be effective for severe gastrointestinal bleeding of HHT.
Go to :
 XML Download
XML Download