

 PDF
PDF ePub
ePub Citation
Citation Print
Print


TO THE EDITOR: Whole-arm translocations are relatively rare cytogenetic aberrations in hematologic malignancies [1]. Mostly, these translocations are unbalanced and accompanied by genomic imbalances, such as trisomy and monosomy of each whole-arm of the 2 involved chromosomes. Until now, approximately 11 different unbalanced whole-arm translocations have been reported as the sole recurrent abnormalities in hematologic malignancies: der(1;7)(q10;q10), der(1;14)(q10;q10), der(1;15)(q10;q10), der(1;18)(q10;q10), der(7;12)(q10;q10), der(13;14)(q10;q10), der(14;21)(q10;q10), der(17;18)(q10;q10), der(1;7)(q10;p10), der(1;7)(p10;q10), and der(9;18)(p10;q10) [1].
Particularly, the der(1;18)(q10;q10) translocation is very rare in hematologic malignancies. Only 3 cases of hematologic malignancy with der(1;18)(q10;q10) translocations have been reported since the translocation was first described by Wan et al.; each was a case of refractory anemia with excess blasts (RAEB), myeloproliferative disorder (MPD), and essential thrombocythemia (ET) [2, 3]. A few other cases including non-Hodgkin's lymphoma (NHL), polycythemia vera, and primary myelofibrosis had der(1;18) (q10;q10) translocations as a part of a more complex karyotype, but lacked detailed case descriptions [1, 4, 5, 6].
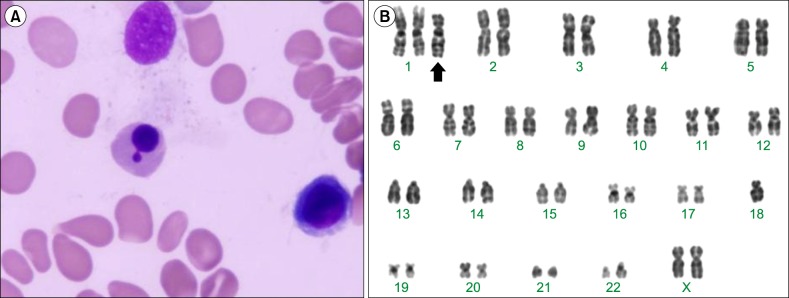
Three years ago, a 73-year-old woman was admitted to our hospital because of pancytopenia. Her complete blood cell count (CBC) showed a hemoglobin (Hb) level of 7.7 g/dL with a mean corpuscular volume (MCV) of 105 fL (reference, 80-99 fL), a platelet count of 58×109/L, and a white blood cell (WBC) count of 2.29×109/L with 40% segmented neutrophils, 46% lymphocytes, 8% monocytes, and 3.9% eosinophils. The peripheral blood smear showed macrocytic erythrocytes without immature cells. At that time, a bone marrow (BM) biopsy was not performed. Theserum vitamin B12 level was 234 pg/mL (reference, 211-911 pg/mL) and the folate level was >20 ng/mL (reference, 4.2-19.9 ng/mL). Despite vitamin supplementation therapy for 3 years, her pancytopenia did not improve. However, her general health status was sustained at a tolerable state. Three months ago, the patient was diagnosed as having gastric adenocarcinoma and underwent a total gastrectomy. At that time, her CBC still showed pancytopenia with the following blood markers: Hb, 9.1 g/dL; WBC, 2.04×109/L (47.6% segmented neutrophils, 40.8% lymphocytes, 6.5% monocytes, and 1.3% eosinophils), and platelets, 58×109/L. The MCV was 102 fL and the serum vitamin B12 level was 1,180 pg/mL. The serum iron, total iron binding capacity, and ferritin levels were 114.1 µg/dL (reference, 29-164 µg/dL), 301 µg/dL (reference, 22-433 µg/dL) and 532.7 ng/mL (reference, 10-291 ng/mL), respectively. The reticulocyte level was 1.83% (reference, 0.5%-1.5%). The BM was hypocellular with 38.6% myeloid cells, 37.0% erythroid cells, and 20.7% lymphocytes. The erythroid series were slightly increased and a mild dyserythropoiesis (megaloblastic changes, binuclarity, and nuclear buddings) was observed (Fig. 1A). Myeloid cells and megakaryocytes were unremarkable in morphology and number. BM iron was sufficient (3+/5+). A BM cytogenetic study revealed the following chromosome abnormalities: 46,XX,+1,der(1;18)(q10;q10)[5]/46,XX[15] (Fig. 1B). As a result of the BM findings and the clonal chromosomal changes, the patient was diagnosed as having unclassifiable myelodysplastic syndrome (MDS-U), according to World Health Organization classification system. Because of her old age and stable general condition, the patient is only receiving vitamin supplementation therapy and is scheduled forregular follow-up visits.
Although a der(1;18)(q10;q10) translocation has been reported in a case of NHL, this translocationis mainly observed in myeloid disorders, primarily in myeloproliferative neoplasms. Moreover, 3 cases including our case had the der(1;18)(q10;q10) translocation as the sole abnormality; this indicates that der(1;18)(q10;q10) might be a primary change in myeloid diseases.
With unbalanced der(1;18)(q10;q10) translocations, either trisomy 1q or monosomy 18p has been suggested to contribute to leukemogenesis. Trisomy 1q may contribute to leukemogenesis through a gene dosage effect as the region q25-q32 has been suggested to give rise to a proliferation advantage of the neoplastic clone in hematologic malignancies [7]. Monosomy 18p may also contribute to clonal proliferation due to the loss of putative tumor suppressor genes. Recently, the l(3)mbt-like 4 (L3MBTL4) gene located on 18p has been proposed to function as a tumor suppressor gene in breast cancer [8]. However, this candidate region and gene should be further evaluated for its role in carcinogenesis.
The prognostic effect of an extra 1q chromosome in myeloid disorders has been variable. While the presence of the der(1;7)(q10;p10) translocation was reported to correlate with leukemic transformation and poor prognosis in MDS [9,10], the der(Y)t(Y;1)(q12;q12) translocation does not lead to a poor prognosis [11]. For cases harboring a der(1;18) (q10;q10) translocation, the prognostic implications were also variable (Table 1). The MPD case showed a very stable clinical course for 2 years [3]. Similarly, the ET case also showed a relatively stable treatment progress. However, the RAEB case displayed an aggressive clinical course and the patient died just 1 month after the initial presentation [3]. In contrast, our case showed a very indolent clinical course. Although our case was diagnosed as having MDS-U just a few months ago, there is a distinct possibility that this patient already had MDS 3 years ago, based on the persistent pancytopenia. This supposition sufficiently supports the indolent progression of the MDS-U with the der(1;18)(q10;q10) translocation.

In conclusion, we report a rare case of MDS-U with a der(1;18)(q10;q10) translocation showing a very indolent clinical progress. Although all but one of the previous cases showed a mild clinical presentation, the prognostic implications of the der(1;18)(q10;q10) translocation cannot be extrapolated at this point due to the very small number of cases. Therefore, the prognostic significance as well as phenotypic variance of the der(1;18)(q10;q10) translocation have to be determined through the collection and analysis of further cases.
 XML Download
XML Download