

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Paraneoplastic syndromes are symptoms arising in cancer-bearing patients due to the local or distant spread of tumors or due to the secretion of hormones or cytokines by the tumor. Although they occur infrequently, their recognition is important because they represent the earliest manifestation of a cancer and mimic metastatic symptoms. Because paraneoplastic syndromes can cause considerable morbidity, early and effective diagnosis and treatment can affect overall clinical outcomes.
Leukocytosis can occur in cancer patients as a result of myeloid growth factor treatment, bone marrow involvement of tumor, or, more rarely, as a paraneoplastic syndrome. Generally, paraneoplastic leukocytosis does not require specific therapy. However, this could be important when treating patients with malignancies to differentiate this cause of leukocytosis from the others, such as infections, allergic reactions, collagen disorders, hematological malignancies, and the side effects of certain drugs like corticosteroid and lithium.
Paraneoplastic leukocytosis presents in combination with several malignancies, including thyroid cancers [1-11]. In Korea, only 1 case of paraneoplastic leukocytosis has been reported so far, and this was associated with uterine cervical cancer [12]. We describe a case of acute pyelonephritis (APN). The patient was also diagnosed with anaplastic thyroid carcinoma with leukocytosis caused by elevated production of granulocyte colony-stimulating factor (G-CSF) by the carcinoma.
Go to : 
CASE REPORT
A 75-year-old woman presented with fever and loss of appetite. She had been treated for diabetes and hypertension for the past 20 years. Four years previously, she had taken levothyroxine sodium (Synthroid) for hypothyroidism, the cause of which was unknown, for several months. As euthyroid state was maintained, she had been taken off medication for the past 3 years and was followed up for simple goiter. She was a non-smoker and had not previously drunk alcohol. Upon physical examination, her body temperature was 37.5℃, her pulse rate was 128 beats/min, and her blood pressure was 110/70 mmHg. She looked chronically ill but was alert. A tender fist-sized, warm, soft mass was observed in the hypochondriac region of the anterior surface of the neck. No specific abnormalities were noted on examination of the chest or abdomen, except for tenderness at the left costovertebral angle.
Laboratory tests on peripheral blood revealed significant leukocytosis (34.9×109/L) with neutrophilia (91%). On peripheral blood smear, neutrophils had normal morphological features and immature cells were not detected. The hemoglobin level was 8.3 g/dL, and the platelet count was 547×109/L. Levels of acute phase reactants were elevated, with erythrocyte sedimentation rate (ESR) of 47 mm/hr and C-reactive protein (CRP) level of 221 mg/L. Other laboratory findings were as follows: blood urea nitrogen, 35.8 mg/dL; serum creatinine, 1.58 mg/dL; serum glucose, 437 mg/dL; total cholesterol, 89 mg/dL; serum sodium, 128 mEq/L; serum potassium, 4.4 mEq/L; serum chloride, 88 mEq/L; serum parathyroid hormone, 58.5 pg/mL; serum calcium, 9.5 mg/dL; and serum albumin, 3.5 g/dL. Urinalysis revealed pyuria (white blood cells [WBC] count >61/HPF).
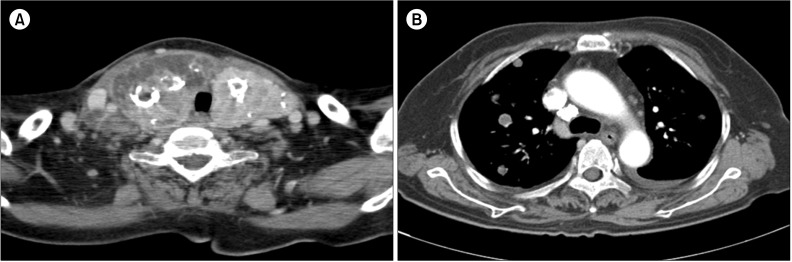
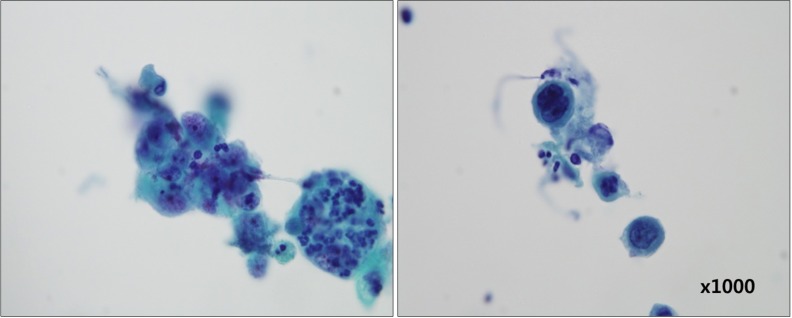
On the basis of these results, APN was diagnosed. While treatment for APN was ongoing, the mass on the patient's neck was examined. Results of the thyroid function test were compatible with sick euthyroid syndrome, considering the patient's seriously ill condition: low T3 levels (16.8 ng/dL), normal T4 levels (8.0 µg/dL), slightly elevated free T4 levels (1.89 ng/dL), and suppressed thyroid stimulating hormone levels (0.02 µIU/mL). Tests for all anti-thyroid autoantibodies, including thyroid stimulating immunoglobulins, anti-thyroglobulin antibody, and anti-microsomal antibody, were negative. Chest radiography showed that both lungs had thyroid lesions with dense calcifications on both sides and multiple nodules. Computed tomography (CT) scan of the neck and chest showed a large thyroid mass and multiple metastatic nodules in both lung fields with cervical, supraclavicular, and mediastinal lymphadenopathy (Fig. 1). Fine needle aspiration of the thyroid mass was performed, and anaplastic thyroid carcinoma was diagnosed following cytological examination (Fig. 2).
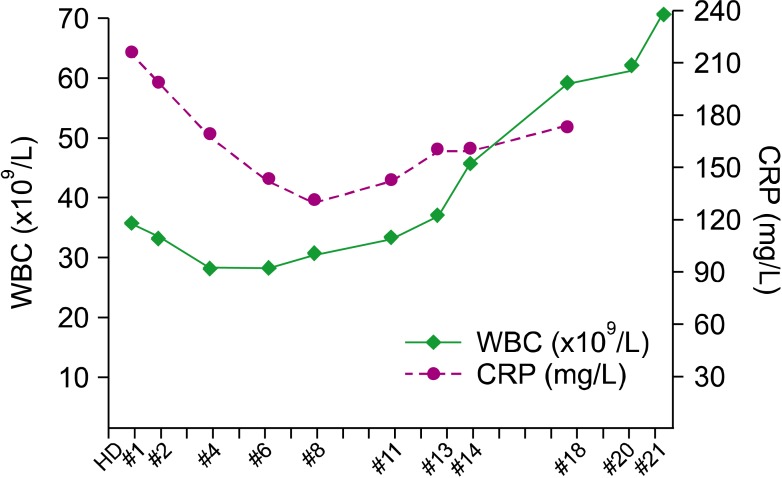
Pyuria and fever were alleviated after administration of 400 mg/day ciprofloxacin for 3 days. On the fifth day of ciprofloxacin administration, treatment was switched to cefotaxime because ciprofloxacin-resistant Escherichia coli was detected in the patient's urine. After cefotaxime administration, bacterial growth was no longer detected in the urine (day 12 of hospital stay). However, the administration of antibiotics did not improve leukocytosis. The WBC count slightly decreased to 28.5×109/L by day 6 of hospital stay, but it steadily increased to 68.8×109/L by day 21 with 91% neutrophils. Although systemic symptoms related to infection improved, no significant increases in other inflammatory markers such as CRP were noted (Fig. 3).
To further investigate this persistent leukocytosis, the serum concentration of G-CSF was measured on day 21 of hospital stay, and it was found to be markedly increased at 1,010 pg/mL (normal range, 3.7-32.3 pg/mL; Quantikine ELISA Kit; R&D System, USA). Despite supportive care, the patient's condition rapidly deteriorated. Respiratory failure developed, and the patient died on day 23 of hospital stay.
Go to :
DISCUSSION
Paraneoplastic leukocytosis was first reported in 1954 [13]. It was defined as elevated peripheral blood leukocyte levels caused by cytokines, likely produced by the tumor itself, without evidence of infection or myeloproliferative disease. The WBC count typically ranges from 12 to 30×109/L and represents neutrophilic leukocytosis with no increase in the proportion of immature forms of neutrophils. Patients with paraneoplastic leukocytosis are often asymptomatic, and cases of paraneoplastic leukocytosis associated with carcinomas of the lung, colon, stomach, kidney, and ovary have been reported.
An increase in human granulopoietic colony-stimulating activity in human lung cancer cell lines was first demonstrated in 1977 [14]. The activity was shown to be dose-dependent on human bone marrow cells [14], although the mechanism of this phenomenon was not clarified. Recently, various cytokines produced by malignant tumor cells have been demonstrated to induce leukocyte proliferation. G-CSF, granulocyte-macrophage colony-stimulating factor (GM-CSF), macrophage colony-stimulating factor, tumor necrosis factor α (TNF-α), interleukin 1, interleukin 3, and interleukin 6 have been shown to be factors capable of inducing marked leukocytosis. These cytokines are known to facilitate the proliferation, differentiation, and mobilization of neutrophils. Survival of patients with paraneoplastic leukocytosis is very poor, despite the administration of appropriate treatment. One study showed that the prognosis of G-CSF-producing lung cancer was worse than that of non-G-CSF-producing lung cancer [15]. Paraneoplastic leukocytosis could also manifest in the late stages of CSF-producing cancers.
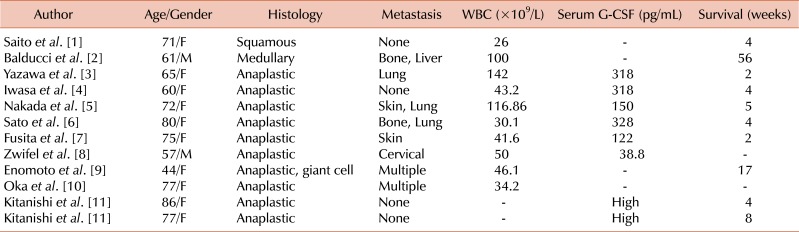
Paraneoplastic leukocytosis has predominantly been demonstrated in lung and gastrointestinal cancers but has also been reported in adenocarcinomas of the breast, brain, ovary, and kidney and in Hodgkin's lymphoma. It rarely occurs in patients with thyroid carcinomas. Table 1 shows the characteristics of reported thyroid carcinomas with paraneoplastic leukocytosis. As in our case, many G-CSF-producing thyroid cancers were anaplastic carcinomas [5], but several cases were squamous or medullary carcinomas [1, 2]. In most cases, patients showed inflammatory symptoms, such as significant elevation of the ESR and CRP levels, without evidence of infection.
Anaplastic thyroid carcinoma is one of the most aggressive human neoplasms and is associated with a high mortality rate. The characteristics of anaplastic thyroid carcinoma are rapid growth beyond the capsule into the adjacent vital structures of the neck and metastasis within 1 year. Various cytokines secreted by human anaplastic thyroid cancer promote the growth of cells [10]. Colony-stimulating factors produced by anaplastic thyroid carcinomas were suggested to have a role in their poor prognosis. Oncogene-induced cytokines, such as GM-CSF, were shown to be important for the development and progression of thyroid carcinoma in animal studies. Furthermore, in a mouse model, CSF-producing tumors were shown to be more likely to metastasize than non-CSF-producing tumors. Hence, it was suggested that paraneoplastic leukocytosis with high levels of G-CSF could be considered a marker of poor prognosis.
In this case, a very high level of serum G-CSF was detected with significant leukocytosis despite improvement in symptoms of infection. As in the other reported cases, rapid progression of disease was noted (Table 1). However, other cytokines related to paraneoplastic leukocytosis such as GM-CSF, TNF-α, and interleukins were not measured. Because of the severity of the patient's condition, sufficient tissue could not be collected for immunohistochemical staining of G-CSF, and therefore, we were unable to directly prove G-CSF production by the tumor itself. G-CSF was thought to originate from the tumor cells because the serum level was remarkably high, even compared to that reported previously, and it caused significant leukocytosis with neutrophilia despite improvement in symptoms of infection.
In conclusion, leukocytosis without definite evidence of infection could be a paraneoplastic manifestation in patients with malignant tumors, including those with anaplastic thyroid cancer. Paraneoplastic leukocytosis could reveal the existence of a tumor producing various cytokines that stimulate hematopoiesis, such as G-CSF, and may be related to poor prognosis.
Go to :
 XML Download
XML Download