

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acute promyelocytic leukemia (APL) is a well known type of acute myeloid leukemia (AML) with characteristic biological and clinical features, which include the presence of the chromosomal translocation t(15;17)(q22;q12) resulting in the fusion of the promyelocytic leukemia (PML) and retinoic acid receptor-α (RARA) genes, the frequent association at diagnosis of a severe hemorrhagic diathesis, and an in vitro and in vivo sensitivity to the differentiating agent all-trans retinoic acid (ATRA) [1-3]. According to the 2008 World Health Organization (WHO) classification [4], the presence of t(15;17) or the gene rearrangement PML-RARA is required to diagnose APL. To date, 3 isoforms of PML-RARA fusion transcripts are known: short (S), long (L), and variable (V) [5].
The current standard for induction therapy is the simultaneous combination of ATRA with anthracycline-based chemotherapy, which results in an extremely high antileukemic efficacy, achieving a 90% to 95% complete remission rate [6, 7]. Because the detection of PML-RARA at diagnosis predicts a response to ATRA [8], diagnostic identification of t(15;17) or PML-RARA is critical for not only the diagnosis of the disease but also the correct therapeutic intervention. In addition, coagulopathy in APL can be life threatening and requires emergent therapy along with a prompt diagnosis by the integration of morphological findings, immunophenotype, cytogenetics, and molecular studies [9].
This study was undertaken to assess the current routine practice in APL, with a focus on whether the genetic test results are available by the time that therapeutic decisions are made. The clinico-pathologic features of APL were also assessed.
Go to : 
MATERIALS AND METHODS
Forty-eight Korean patients, who were newly diagnosed with APL between March 2007 and February 2012 in 5 university hospitals, were included in this study. We reviewed the clinical and laboratory findings of the patients, such as age, gender, complete blood cell (CBC) counts, prothrombin time (PT), activated partial thromboplastin time (aPTT), fibrin/fibrinogen degradation product (FDP), D-dimer, bone marrow (BM) study, immunophenotyping, chromosome analysis, molecular study, and therapeutic regimens administered. We also investigated the turnaround time (TAT) of laboratory tests confirming the presence of t(15;17) (chromosome analysis) or PML-RARA (molecular study), and the elapsed time between the initiation of induction therapy and the BM study. The TAT was defined as the time interval between the receipt of a bone marrow sample at the laboratory and the verification of the test results.
This study was performed under the approval of Ajou University Hospital Institutional Review Board. The flow cytometric analysis for immunophenotyping, chromosome analysis, and molecular studies were carried out according to the same methods as our previous study [10].
Go to :
RESULTS
The demographic characteristics and laboratory features of the 48 APL patients are summarized in Table 1. All the patients were adults except for one. Prolonged PT was observed in 38 (81%) out of 47 patients tested, and prolonged aPTT in 6 patients (13%). Increased FDP and D-dimer were observed in all of the 39 patients tested.
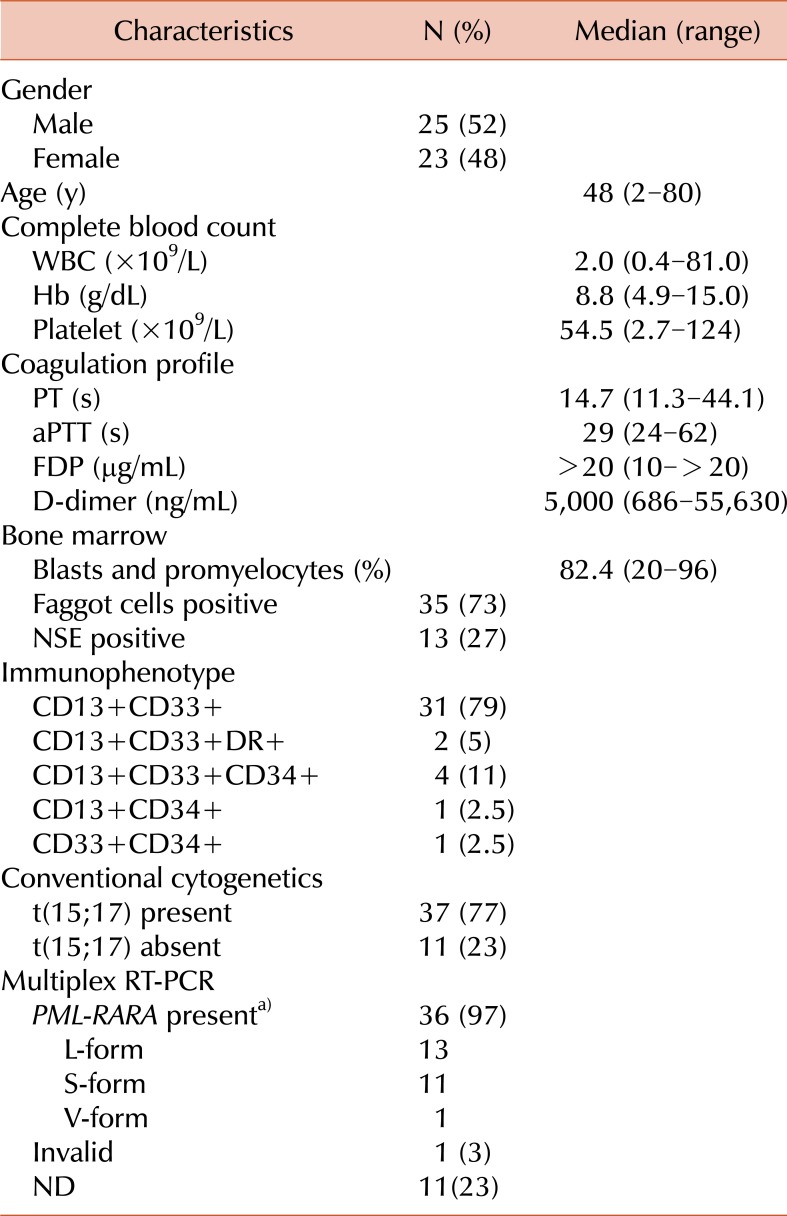
Table 1
Demographic & laboratory characteristics of the 48 patients with acute promyelocytic leukemia.
a)While presence of PML-RARA was confirmed in 36 patients, PML-RARA isoform results were available in 25 cases.
Abbreviations: WBC, white blood cell; Hb, hemoglobin; PT, prothrombin time; aPTT, activated partial thromboplastin time; FDP, fibrin/fibrinogen degradation product; NSE, nonspecific esterase; RT-PCR, reverse transcriptase-polymerase chain reaction; ND, not done.
![]()
The results of fluorescent in situ hybridization (FISH) were only available for 13 patients and were not included in this study.
Immunophenotyping: The strong expression of CD33 was a constant feature in all patients, and it was accompanied by variable CD13 expression. All patients but 2 (44/46, 96%) showed the characteristic absence or a low percentage of HLA-DR expressing cells. Only 6 patients (13%) were CD34 positive.
Conventional cytogenetics: Among the 48 patients, the t(15;17) translocation was found in 37 patients (77%), a normal karyotype in 9 patients (19%), 45,X,-Y in one patient (2%), and 47,XY,+8 in one patient (2%). The reverse transcriptase-polymerase chain reaction (RT-PCR) detected PML-RARA in all 11 patients whose karyotyping failed to reveal t(15;17). Sixteen cases (33%) had additional chromosomal abnormalities besides t(15;17) (Table 2). The most common additional chromosomal abnormality was +8. The median TAT for chromosome analysis was 7 d (Table 3).
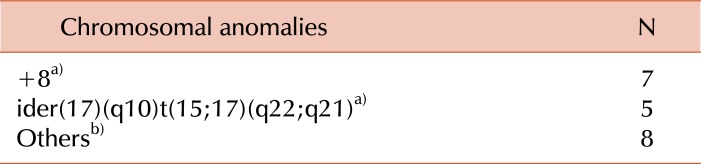
Table 2
Additional chromosomal abnormalities in APL patients.
a)Two patients had both trisomy 8 and ider(17)(q10)t(15;17)(q22;q21), one patient had trisomy 8 and del(6)(q21q25), and one patient had trisomy 8 and add(6)(q27). b)Other abnormalities include t(2;14)(q11.2;q11.2)del(11)(q23)/t(7;14)(p10;q10),-14/16q-/inv(9)(p12q13)/del(6)(q21q25)/+21/+6(q27)/add(19)(p13.3).
![]()
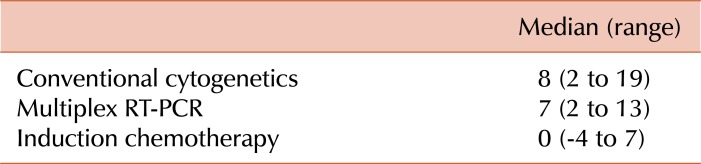
Molecular studies: Multiplex RT-PCR for PML-RARA isoforms was performed in 37 out of 48 patients, and PML-RARA was detected in 36 cases (Table 1). RT-PCR failed to yield a valid result in one case because there was no amplification of the internal control fragment. The cytogenetic study detected t(15;17) in the 12 cases whose RT-PCR results were invalid or unavailable. The median TAT for RT-PCR was 7 d (Table 3).
Induction therapy: Induction regimens given to the APL patients were as follows: ATRA alone (N=11, 26%), ATRA+idarubicin (N=25, 58%), ATRA+cytarabine (N=3, 7%), and ATRA+idarubicin+cytarabine (N=4, 9%). The median time interval between the BM study and the initiation of induction therapy was 0 d (Table 3).
Go to :
DISCUSSION
APL is uncommon in children under 10 years of age and is mostly prevalent in midlife. Most of the demographic and laboratory characteristics of our patients (Table 1), including immunophenotype and distribution of PML-RARA isoforms, do not seem to differ substantially from those of previous reports [11-15]. Flow cytometric analysis is a useful tool in helping to make a correct diagnosis. Strong CD33 expression, CD13 positivity, and a lack of HLA-DR expression were characteristic findings in almost all patients studied. Only 2 patient (2%) showed an HLA-DR expression, which has been reported in up to 6% of APL patients [13, 16, 17].
All 48 patients revealed the markers t(15;17) or PML-RARA by conventional cytogenetics, RT-PCR, or both. Therefore, a combination of chromosome analysis and RT-PCR is ideal for diagnosing APL [18]. In addition, RT-PCR has been used as the only technique that defines the PML breakpoint type in PML-RARA fusion genes. This defines an appropriate strategy for subsequent minimal residual disease (MRD) monitoring [19] although Lee et al. showed that the PML-RARA isoform type made no significant difference in pretreatment clinical characteristics or treatment outcomes [14].
In previous studies, secondary cytogenetic abnormalities have been reported in 26% to 40% of cases, and among them, trisomy 8 was reported as the most frequent abnormality, with ider(17)(q10) accounting for only 1% to 3% [20, 21]. However, in the present study, ider(17) was observed in 5 patients (10.4%), being the second most frequently observed additional chromosomal abnormality following trisomy 8. Although the significance of this finding remains to be fully elucidated, it is noteworthy that ider(17) is one of the most common additional chromosomal aberrations in the Korean population.
Ever since the introduction of ATRA in front-line therapy APL has been considered to be the most curable subtype of AML [22, 23]. Despite the great improvement in APL treatment, early death due to severe bleeding is one of the major problems in APL, which occurs in approximately 5-10% of newly diagnosed cases [24]. The life-threatening bleeding problems associated with disseminated coagulopathy require instant treatment with ATRA, and the correct diagnosis should be considered as a medical emergency in a patient with APL, requiring a fast and accurate diagnosis, preferably within hours [25].
However, the genetic (molecular) techniques are time consuming: 1-2 d for FISH and PCR techniques and even 1-2 weeks for cytogenetics [25]. Our results confirmed the current practice that chromosome analysis required a median of 7 d (minimum 2 d, maximum 19 d) and RT-PCR, 7 d (minimum 2 d, maximum 13 d) (Table 3). Although RT-PCR might require 2-3 d, we realized that RT-PCR was being performed on a weekly basis due to the limited numbers of well-trained technicians and PCR machines, which resulted in the disappointingly long TAT of RT-PCR.
The present study showed that induction therapy required a median of 0 d because most patients started the therapy on the same day that the BM study was conducted. The decision to start therapy was made depending mainly on the morphology, cytochemical reaction, and/or immunophenotype of the leukemic blasts. In practice, hematologists tend to start induction therapy with an unknown state of t(15;17) or PML-RARA because late diagnosis and delayed treatment initiation are significantly associated with severe bleeding and early death in APL [26]. Therefore, an atypical morphology or immunophenotype may compromise a rapid diagnosis and treatment of APL.
The current practice seems too slow and time consuming for routine diagnostic applications and needs to be improved in the detection of the characteristic oncogene or oncoprotein. To improve the clinical and laboratory flow, it might be necessary to introduce a much faster technique that can be performed more easily and without special laboratory facilities, as well as a more meticulous management of skills to adjust and prioritize the laboratory processes. A promising new method called the PML-RARA immunobead assay, which adopts a faster and easier flow cytometric technique and immunobead-based detection of the fusion protein, has shown fully concordant results with RT-PCR [25]. We herein highlight the continued requirement for faster assays to be made available for routine laboratory use as soon as possible.
In summary, our study showed that the results confirming the presence of t(15:17) or PML-RARA are not available at the time of decision for treatment in most APL cases because the cytogenetic and molecular tests require highly technical and time-consuming procedures that are not available in all locations due to resource limitations. Since APL represents a medical emergency, and accurate diagnosis is a prerequisite for prompt treatment, faster diagnostic tools to confirm the presence of PML-RARA are urgently required in routine laboratories in order to reduce mortality from APL.
Go to :
 XML Download
XML Download