

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Posterior reversible encephalopathy syndrome (PRES) is a transient clinicoradiologic phenomenon characterized by seizure, headaches, altered mental status, and visual impairment with abnormal signal lesions on magnetic resonance imaging (MRI). Since it was first proposed in 1996 by Hinchey et al. [1], PRES has been reported in various conditions, such as renal disease, eclampsia, autoimmune disease, hematologic-oncologic malignancies, transplantation, and sepsis [2-14] and has developed in association with the use of medications such as chemotherapeutic agents, immunosuppressive drugs, immunoglobulin, and antiangiogenic drugs [15-17].
PRES may occur in patients being treated for hemophagocytic lymphohistiocytosis (HLH), which is a life-threatening disease characterized by a generalized proliferation of histiocytes as a result of ineffective, uncontrolled activation of cytotoxic T cells and antigen-presenting cells and up-regulation of inflammatory cytokine [18, 19]. HLH has usually been treated since 2004 according to the international Histiocyte Society treatment protocol (HLH-2004), which includes etoposide, dexamethasone, and cyclosporin A (CSA) and, in selected patients, intrathecal therapy with methotrexate and corticosteroids to provide more intensive immunosuppression at the beginning of treatment [20].
We have observed significant neurologic toxicity, which is proposed to be PRES, during treatment with the HLH-2004 protocol. Because HLH is a rare multisystem disorder, in which the occurrence of PRES is even rarer, it can be difficult to distinguish PRES from other neurologic manifestations. However, careful differential diagnosis of these neurologically toxic conditions from other causes of neurologic conditions is necessary, especially with central nervous system (CNS) involvement of hemophagocytosis. HLH is frequently associated with CNS lesions with highly variable clinical manifestations at onset or during progression, and delayed diagnosis may result in permanent damage to the affected brain tissues with poorer outcomes, contrary to PRES [21].
In this study, we analyzed the clinical and laboratory findings, radiologic features, and long-term outcomes of patients with HLH who developed PRES during treatment using the HLH-2004 protocol and evaluated the role of putative risk factors for prediction of PRES related to HLH.
MATERIALS AND METHODS
Patients
We retrospectively reviewed the medical records of 28 patients who had a diagnosis of HLH and were treated according to the HLH-2004 protocol in the Department of Pediatrics at Ewha Womans University Mokdong Hospital, Seoul, Korea between April 2005 and April 2012. Six of these patients had a diagnosis of HLH and were treated for PRES, and they were enrolled in this study. One of these 6 patients repeatedly experienced PRES during 2 separate treatments due to reactivation of HLH, so a total of 7 events of PRES in 6 patients were reviewed.
Methods
All 28 patients had a diagnosis of HLH according to the diagnostic criteria proposed by the HLH-2004 protocol, meeting 5 of the following 8 criteria: (1) fever; (2) splenomegaly; (3) cytopenia in 2 or more cell lines (hemoglobin level <9 g/dL, platelet count <100×109/L, and neutrophil count <1.0×109/L); (4) hypertriglyceridemia (≥265 mg/dL) or hypofibrinogenemia (≤150 mg/dL); (5) the presence of hemophagocytosis in the bone marrow, spleen, and lymph node; (6) hyperferritinemia (≥500 ng/mL); (7) an impaired function of natural killer cells or its absence; and (8) a concentration of serum soluble CD25 (soluble interleukin-2 receptor) ≥2,400 IU/mL [5]. All patients were also treated according to the HLH-2004 protocol with combinations of CSA, dexamethasone, and etoposide [20].
PRES was defined by the presence of at least one of the classic clinical symptoms of seizure, headaches, altered mental status, or visual impairment in combination with typical radiologic findings on T2 and fluid attenuation inversion recovery (FLAIR) MRI, including mainly bilateral posterior subcortical hyperintensities. All patients underwent both MRI of the brain and analysis of cerebrospinal fluid (CSF) at diagnosis of HLH and at onset of PRES. None of the 6 patients had abnormal findings at diagnosis of HLH.
We reviewed the medical records of all 28 patients with HLH, including medical history, clinical characteristics, blood pressure, CSF findings, laboratory findings, MRI results, and treatment outcomes at diagnosis and during the clinical course. We compared various clinical and laboratory findings between patients without and with PRES to evaluate putative risk factors related to development of PRES.
Statistical analysis
All analyses were performed using SPSS version 17.0. The Wilcoxon rank sum test and chi-square test were used for comparison of continuous variables between patients with and without PRES. For analysis of putative factors on the development of PRES, chi-square test, Fisher exact test, and logistic regression analysis were performed using selective parameters. Statistically significant variables on univariate analysis were included in a multivariate analysis. A P value <0.05 was considered statistically significant.
RESULTS
Clinical characteristics at the onset of PRES
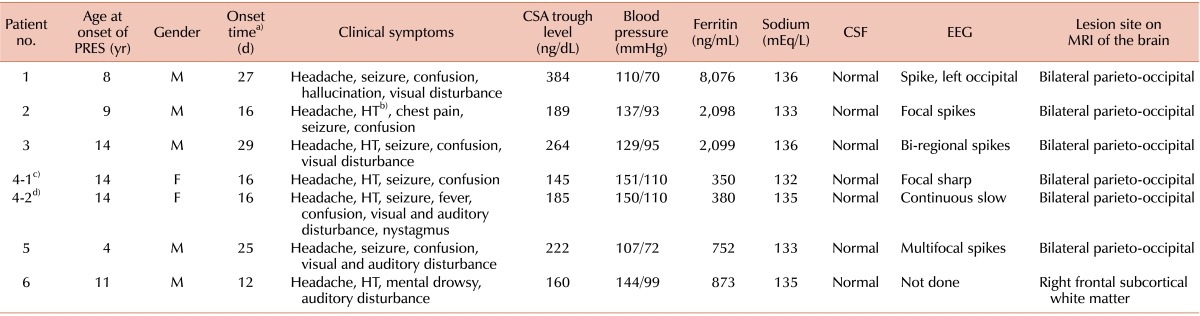
Six of the 28 patients with HLH (21.4%) had documented PRES. Table 1 shows the clinical and laboratory findings of these 6 patients. One patient (patient 4), who was treated with 2 separate cycles of chemotherapy because of reactivation, experienced PRES twice during each HLH treatment. The mean time to development of PRES was 20.1 days (range, 12-29 days) from the start of chemotherapy. All patients experienced various forms of seizures, such as generalized tonic-clonic seizure of gaze deviation, suggesting partial seizure. Before the onset of seizures, all 6 patients experienced headache and altered mental status such as somnolence, drowsiness, and delirium. Four of the 6 patients developed hypertension and visual disturbances such as diplopia and cortical blindness, and 2 of the 6 patients experienced an auditory abnormality.
Laboratory and radiologic findings
The WBCs, results of coagulation studies and fibrinogen assay, liver and kidney function, and calcium and magnesium levels were normal in all patients (data not shown) during PRES. However, hyponatremia (<135 mEq/L) was noted in 3 of the 6 patients. CSA levels were in the therapeutic range, with a mean blood level of 221.3 ng/dL (range, 145-384 ng/dL). Serum ferritin levels were variable in each patient, ranging from 350 to 8,076 ng/dL at the onset of PRES (Table 1).
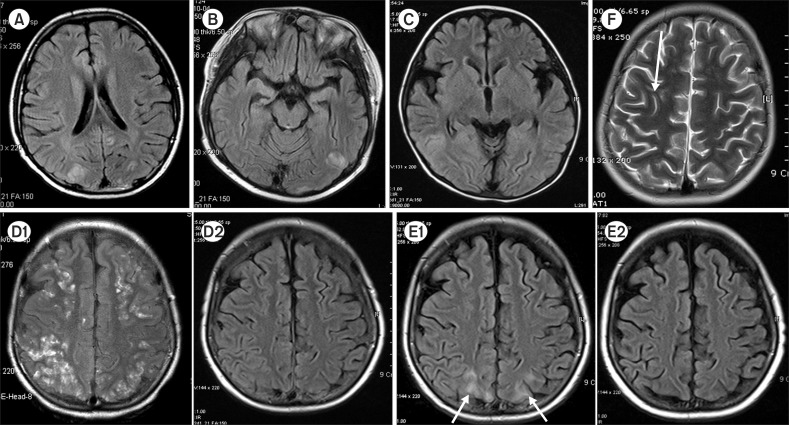
All patients underwent electroencephalography (EEG), CSF analysis, and MRI immediately after neurologic symptoms developed. The results of CSF analysis were normal in all patients with PRES. All patients had abnormal findings on EEG with non-specific slow wave to multifocal spike except for 2 patients (patients 1 and 6) who were not assessed because of their worsening condition (Table 1). MRI showed a decreased signal with a T1-weighted image and hyperintense abnormalities on T2-weighted and FLAIR images typical of PRES bilaterally in the subcortical white matter and cortical gray matter of the posterior parietal and occipital lobes (Fig. 1).
Clinical course and long-term outcomes
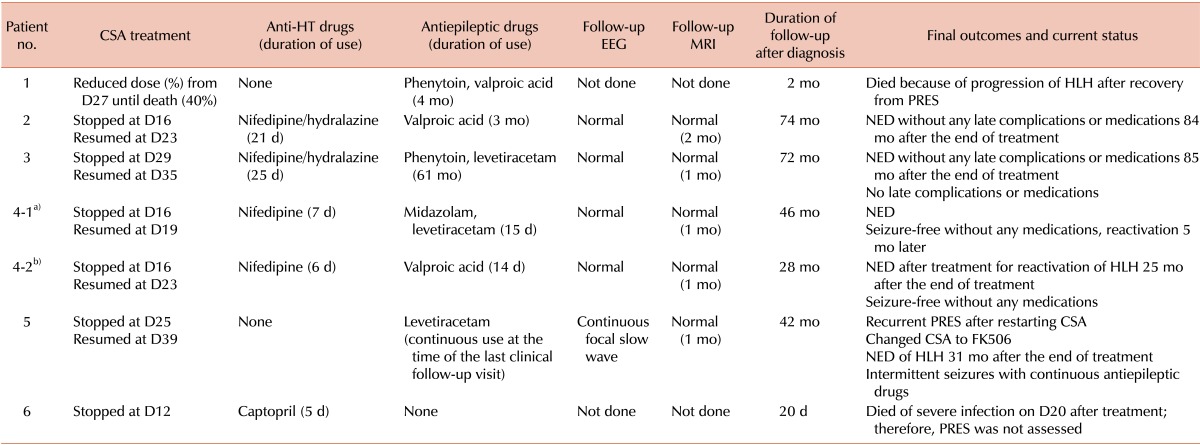
Table 2 shows a summary of the clinical course and long-term outcomes after development of PRES. All patients started treatment for acute seizures with midazolam, phenytoin, valproic acid, or levetiracetam and for hypertension with a calcium channel blocker and/or hydralazine, which succeeded in controlling these conditions. After confirming typical MRI findings for PRES and negative results of CSF analysis, we temporarily discontinued treatment with CSA for 7 to 14 days or reduced the dose because we considered CSA to be a possible cause of the convulsive encephalopathy.
After provision of the supportive care described in the preceding text, the symptoms of headache, visual disturbance, and altered mental function slowly improved and resolved in all patients, as shown by normal findings on neurologic examinations in the subsequent 1 to 2 weeks. All patients showed no aggravation of HLH during temporal cessation of treatment with CSA. Four of the 6 patients resumed treatment with CSA within 7 or 14 days after diagnosis of PRES under careful medical observation, and 5 of the 6 patients tolerated CSA well without recurrence of neurotoxicity when CSA therapy resumed. However, 1 patient (patient 5) developed the same symptoms relating to PRES 2 days after restarting CSA therapy, and CSA was changed to FK506 after his medical condition was stabilized. This patient successfully completed chemotherapy with FK506 without recurrence of PRES and reactivation of HLH. Another patient (patient 4) experienced a second occurrence of HLH while undergoing treatment for reactivation with the same HLH-2004 protocol, and her condition was successfully managed with CSA with temporal withdrawal. Patient 1 was being treated with a 20% reduction of the original dose of CSA at diagnosis of PRES, and the dose was reduced by 10% every week to a 40% reduction of the dose until the patient's death.
All patients were able to discontinue treatment with antihypertensive drugs within 7 to 25 days after onset of PRES. Antiepileptic drug therapy was maintained for several months until confirmation of complete recovery, which was based on normal findings on follow-up EEG after full recovery from the seizure attack and seizures were well controlled even after cessation of drug therapy. One patient (patient 5) continued long-term treatment with an antiepileptic drug at the time of his last clinical follow-up visit because of repeated seizure episodes even though no epileptiform discharges were noted on EEG.
Follow-up MRI showed complete recovery to normal in all patients between 1 and 2 months (median, 1.2 months) except for 2 patients (patients 1 and 6) who were not assessed by MRI (Fig. 1, D2 & E2). The patient who continued long-term treatment with an antiepileptic drug (patient 5) had normal findings on MRI 1 month later.
All patients recovered without any residual symptoms of PRES except for 1 patient who died of HLH-related complications after recovery from PRES.
Putative risk factors for patients with HLH who developed PRES
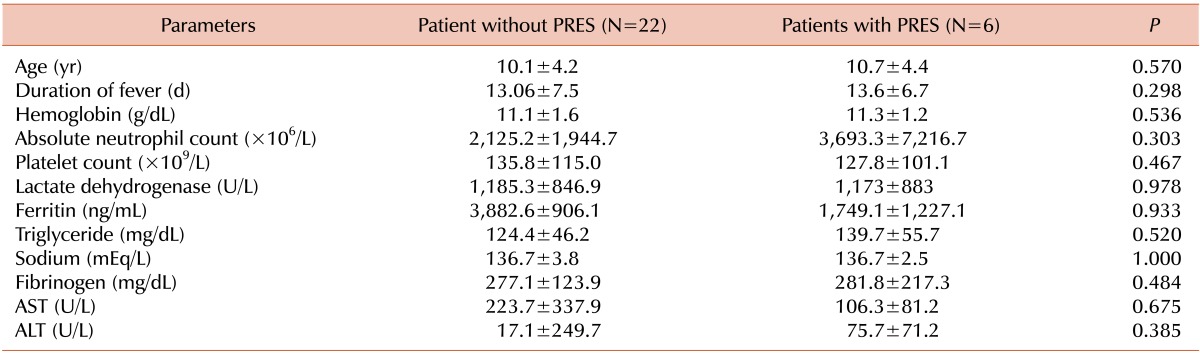
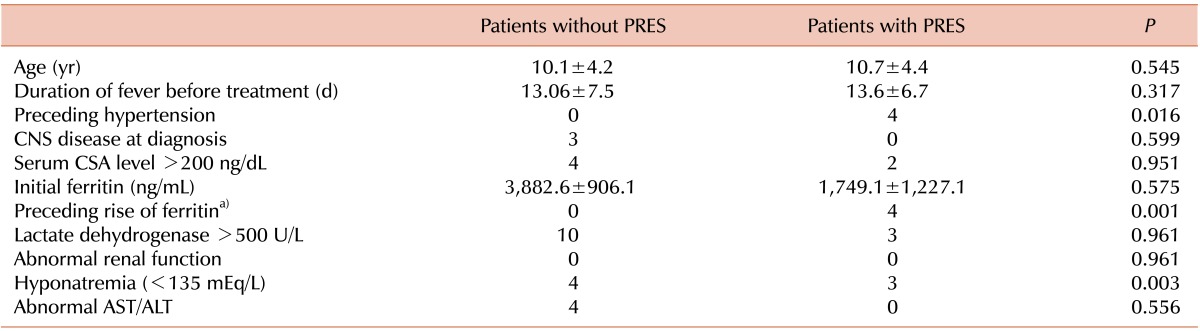
We compared the clinical and laboratory findings at diagnosis of HLH between patients with and without PRES to determine the putative risk factors. The clinical and laboratory findings were not statistically different in both groups (Table 3). We also performed logistic regression analysis using selective clinical and laboratory parameters. Among the several factors, preceding hypertension (P=0.016), a preceding rise in ferritin level >50% compared with 1 week before development of PRES (P=0.001), and hyponatremia (<135 mEq/L) (P=0.003) were statistically significant (Table 4). These factors apparently comprise putative risk factors for PRES complicated during induction chemotherapy compared with other factors.
DISCUSSION
PRES is a neurologic complication in pediatric patients undergoing treatment for HLH with the HLH-2004 protocol, although PRES has been described in numerous medical conditions. Previous pediatric studies have reported that most cases of PRES develop during the treatment of children with various cancers, mainly leukemia, and renal dysfunction [2, 8-14].
The incidence of PRES in patients undergoing treatment of HLH is undefined, and there are only 2 reports of PRES related to treatment of HLH thus far [19, 22]. In the present study, PRES was documented in 6 of 28 patients (21.4%) undergoing treatment of HLH. Similar results were reported by Thompson et al. [19], who found that 24% (4/17) of patients treated for HLH had PRES. The overall incidence of PRES varies from 0.49% in patients undergoing solid organ transplantation [23] to 47.4% in pediatric patients with acute lymphoblastic leukemia [9]. When we consider the results of Thompson et al. [19] and our study, HLH might predispose patients to develop PRES and the estimated incidence of PRES-related HLH treatment may be fairly high compared with other conditions causing PRES.
Although the pathophysiology that underlies the development of PRES is likely multi-factorial, the mechanism of PRES has been explained by both vasogenic and cytotoxic effects. Hypertension is one of the main mechanisms proposed [13, 24, 25]. The acute rise of blood pressure leads to vasoconstriction in the cerebral blood vessels as a result of physiologic auto-regulation. However, sustained hypertension leads to the disturbance of cerebrovascular auto-regulation, the dilation of cerebral arterioles, the opening of endothelial tight junctions, and the leakage of plasma and red blood cells into the extracellular space. Finally, edema and micro-infarcts develop (vasogenic theory).
A direct toxic effect on the vascular endothelium (e.g., by different chemotherapeutic agents) is also a proposed mechanism of PRES (cytotoxic theory). Endothelial dysfunction and blood-brain barrier disruption lead to the leakage of plasma and red blood cells into the extracellular space [25, 26].
In our study, 4 of the 6 patients (66.7%) had hypertension before the development of PRES, and preceding hypertension was a significant putative risk factor for PRES (Tables 1 and 4). Therefore, we suggest that hypertension plays a crucial role in the development of PRES in patients with HLH. Hypertension always accompanies PRES as a contributory factor, but some cases of PRES have occurred in patients with normal blood pressure. Two cases of PRES occurred in patients with normal blood pressure in our study, and approximately 30% of cases of PRES were reported in patients with normal blood pressure in the literature [8].
Hypertension is caused by use of the HLH-2004 protocol and the highly inflammatory environment of HLH. Patients with HLH may have higher-risk environments, predisposing them to develop PRES. Our patients were treated according to the HLH-2004 protocol, which is based on etoposide, dexamethasone, and CSA, and the combination of these drugs may increase the incidence of PRES in patients with HLH. CSA, a calcineurin inhibitor, has been considered one of the promoting factors for the development of PRES. CSA neurotoxicity is frequently reported in the setting of both hematopoietic stem cell and solid organ transplantation. The mechanisms of CSA neurotoxicity are unknown, but CSA causes reversible ischemic disturbances in the brain by endothelial cell damage and vasoconstriction [27]. Furthermore, the combination of CSA and dexamethasone may potentiate the risk of developing PRES in patients with HLH via hypertension. Corticosteroids may play an indirect role in the development of PRES due to the higher risk of hypertension, and corticosteroid-induced PRES was reported by Irvin et al. [28]. The CSA level does not seem to compromise predisposing factors, because our patients who developed PRES had a therapeutic range of CSA with a blood level of 221.3 ng/dL (range, 145-384 ng/dL). High CSA blood levels are widely known to be more frequently associated with a high prevalence of PRES, but CSA-associated PRES has also been found in patients with a therapeutic range [22, 29].
Thompson et al. [19] proposed changing the protocol for treatment of HLH regarding early introduction of CSA, which may increase the risk of PRES (41.2% vs. 7.1%), although the difference between the 2 study groups did not quite reach statistical significance. In the HLH-2004 protocol, initiation of cyclosporine was moved from after week 8 to day 1 to provide more intense upfront immune suppression to increase the survival of patients with HLH [20]. We could not compare the risk of PRES according to different study protocols because enrolled patients were treated with the HLH-2004 protocol, not the HLH-94 protocol, but this hypothesis is quite persuasive when we consider the mechanisms of the possible predisposing factors and the higher incidence of PRES in our study compared with other groups at risk for PRES.
Another possible cause of the increased prevalence of PRES in patients with HLH is related to the highly pro-inflammatory state, because HLH is a syndrome of toxic immune activation driven by the interaction of T cells and innate immune cells. As a result, greater amounts of inflammatory cytokines may affect the blood-brain barrier, and the patient might be at greater risk for neurologic toxicity by the mechanism of the vasogenic theory. Our finding that ferritin level is a significant putative risk factor for PRES supports it (Table 4).
We demonstrated that PRES is reversible in patients with HLH and that these patients have favorable outcomes with prompt diagnosis and treatment. Our patients recovered with supportive care, including control of blood pressure, use of antiepileptic drugs, and temporarily reduced or withdrawn treatment with CSA without substitution. None of the patients were observed to have aggravation of HLH during cessation of treatment with CSA, and reintroduction of CSA was well tolerated without recurrence of neurotoxicity in all patients except one (patient 5). Patient 5 redeveloped PRES after restarting treatment with CSA, and we changed CSA to tacrolimus even though tacrolimus may be associated with similar neurotoxic adverse events [30, 31]. Nevertheless, this patient successfully completed treatment of HLH, and his condition has been stable for 42 months (Table 2). All patients with PRES except one (patient 5) discontinued follow-up. All patients had evidence on follow-up MRI 1 month after diagnosis that their brain lesions regressed completely.
In conclusion, PRES has been shown to develop in patients undergoing treatment with the HLH-2004 protocol. The mechanisms of PRES in patients with HLH are related to hypertension resulting from treatment, not disease. However, a hyper-proinflammatory condition in patients with HLH may influence the increase in risk for induction of PRES by potentiating the neurotoxic effect of CSA and dexamethasone. Therefore, our experience indicates that patients receiving treatment that follows the HLH-2004 protocol should be closely monitored for the development of PRES. Awareness of this syndrome is important to distinguish PRES from other neurologic manifestations, especially CNS involvement of hemophagocytosis, and avoid unnecessary treatment or delays and anxiety. Early recognition and proper supportive care can result in a fast recovery without significant long-term sequelae in most patients with HLH. Further evaluation in a larger population is warranted to validate the risk factors suggested in this study.
 XML Download
XML Download