

 PDF
PDF ePub
ePub Citation
Citation Print
Print


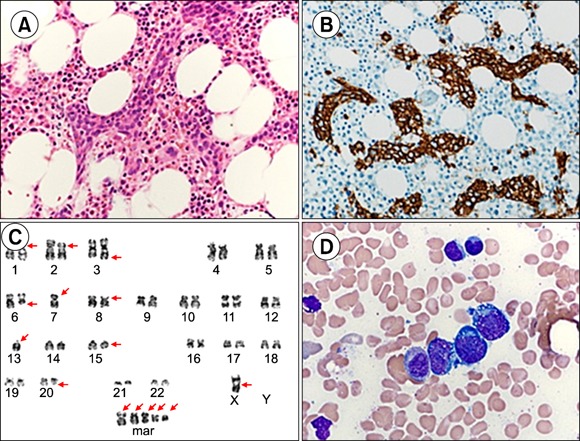
A 44-year-old woman presented with myalgia and fever. Initial laboratory results were: White blood cell (WBC) count, 7.8×109/L; hemoglobin, 11.3 g/dL; platelet count, 42×109/L; and lactate dehydrogenase, 619 IU/L. Peripheral blood cell morphology showed leukoerythroblastic features (nRBC, 8/100 WBCs). Abdominal computed tomography (CT) indicated hepatosplenomegaly. Bone marrow biopsy showed focal large cell aggregates with prominent nucleoli in capillaries (A, H&E stain, ×400; B, CD20 stain, ×400). These cells were positive for CD5 and CD20 and negative for CD10, CD56, CD117, CD34, TDT, and CD3. Chromosomal study showed a complex karyotype (C, 48,-X,add(X) (p11. 2 ) ,add(1)(p12),add(2)(p11.2),add(3)(q27),del(6)(q21) -7,add(8)(p21) , -13,del(15)(q11.2q15) , del(20)(q13.3),+mar1,+mar2,+mar3,+mar4,+mar5[cp3]/46,XX[17]). She was diagnosed with intravascular large B-cell lymphoma and treated with rituximab, cyclophosphamide, adriamycin, vincristine, and prednisolone (R-CHOP) combination chemotherapy. Three months after auto-peripheral blood stem cell transplantation, she was readmitted due to coughing, sputum, and myalgia. Bone marrow analysis showed an intravascular large B-cell lymphoma recurrence with normal karyotype (D, Wright-Giemsa stain, ×1,000). In a BCL6 dual-color, break-apart probe (Vysis/Abbott Molecular, Des Plaines, IL, USA) initial diagnostic specimen FISH study, 9.8% (49/500) of the cells had a 2-green 1-fusion abnormal signal pattern, suggesting 3q27 rearrangement, while no abnormal signal patterns were observed, although abnormal lymphoid cells comprised 6.8% of the bone marrow at relapse.
 XML Download
XML Download