

 PDF
PDF ePub
ePub Citation
Citation Print
Print


TO THE EDITOR: Lymphoplasmacytic lymphoma (LPL) is a neoplasm of small B lymphocytes, plasmacytoid lymphoid cells, and plasma cells that usually involves bone marrow, and sometimes, the lymph nodes and spleen; which does not fulfill the criteria for any other small B cell lymphoid neoplasms that may also have plasmacytic differentiation [1]. Waldenstrom's macroglobulinemia (WM) comprises a significant proportion of LPL cases and is characterized by bone marrow involvement and an IgM monoclonal gammopathy of any concentration [2].
When WM was first described, the general belief was that it did not extend to the skeletal system. However, following several reports of lytic bone lesions in WM [3-6], this belief has been challenged. It is now considered that bone involvement in WM may not be unusual. The abnormal feature that was commonly observed in these previously reported cases was the presence of a predominant plasmacytic morphology in the bone marrow of the WM patients with lytic bone lesions. Contrary to these reports, we hereby report a rare case of WM with lytic bone lesions, showing a predominant presence of lymphocytic infiltration of the bone marrow, and very few plasmacytic cells.
CASE
A 65-year-old male patient, who had a 10-year history of hypertension and type II diabetes mellitus, presented with complaints of pain and a tingling sensation in both lower limbs over the previous year and in both upper limbs over the previous 6 months. He also had a history of weight loss and an intermittent low-grade fever during the previous 6 months.
On examination, the patient was pale, conscious, alert, and oriented with a pulse of 72 beats per minute and blood pressure at 140/90 mmHg. Nothing unusual was found on examination of the chest and cardiovascular systems. Abdominal examination revealed mild hepatomegaly without splenomegaly. Examination of the nervous system showed normal mental status (patient was conscious and well oriented in time, place, and person). Sensations were diminished below the knees in both lower limbs. Power in all of the muscles was 4/5. Fundoscopy revealed a grade 4 hypertensive retinopathy.
Investigations revealed pancytopenia and normocytic normochromic anemia with a hemoglobin of 6.8 g/dL; a total leukocyte count of 1.5×103/mm3; a differential leukocyte count with 23% neutrophils, 71% lymphocytes, 5% monocytes, and 1% eosinophils; a platelet count of 21,000/mm3; and a markedly raised erythrocyte sedimentation rate of 140 mm/hr. Biochemical investigations provided the following results: blood sugar, 92 g/dL; total bilirubin, 0.6 mg/dL; alkaline phosphatase/aspartate transaminase/alanine transaminase, 126/74/55 IU/mL; blood urea, 74 mg/dL; serum creatinine, 1.7 mg/dL; and serum uric acid, 11 mg/dL. The serum protein level was 10.0 g/dL, albumin level was 1.76 g/dL, and the albumin/globulin ratio was 0.2 (reference range, 0.9-2.0). Serum calcium levels ranged from 8.4 to 9.2 mg/dL on different occasions. The venereal disease research laboratory (VDRL), antinuclear antibody, and rheumatoid factor tests were negative, while C-reactive protein was raised. The Coombs test and the test for cold agglutinins were also negative. In addition, the serological markers for hepatitis B and hepatitis C were negative. The skull radiograph revealed multiple lytic lesions.
The chest radiograph showed cardiomegaly with prominent bronchovascular markings. Ultrasonography revealed mild hepatomegaly (15.5 cm in size), while the spleen and both kidneys were within normal limits. The wall of the rectum and sigmoid colon demonstrated thickening. Contrast enhanced computed tomography (CECT) revealed atrophy of the brain and multiple lytic lesions in the skull. The rectal wall was also edematous. There was mild hepatomegaly with the presence of minimal ascites. A clinical diagnosis of multiple myeloma was considered due to the presence of lytic bony lesions, increased total protein values, decreased serum albumin, and low albumin to globulin ratio.
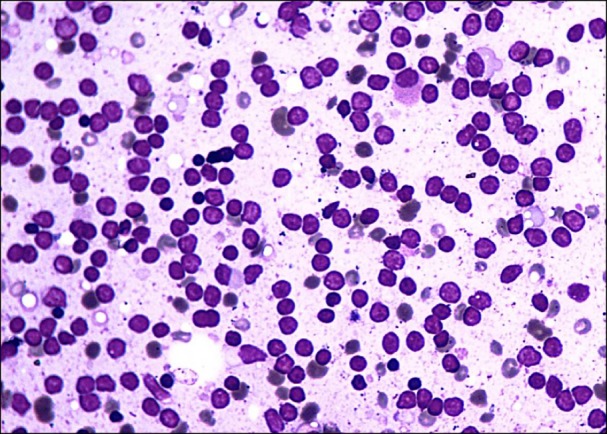
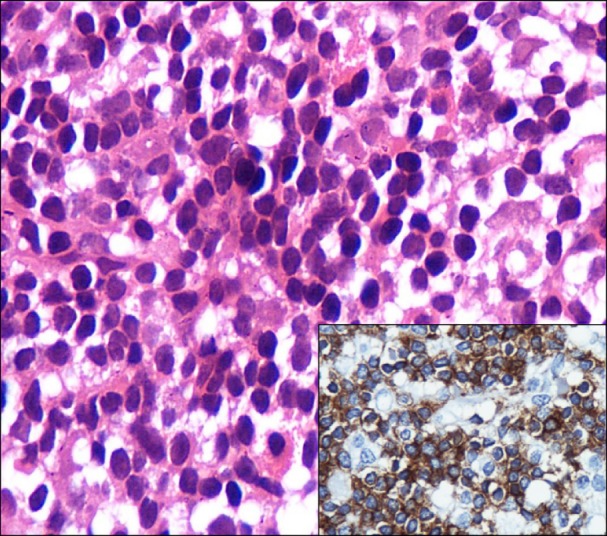
Bone marrow aspiration, bone marrow biopsy, and serum protein electrophoresis were simultaneously performed to confirm the diagnosis of multiple myeloma. Bone marrow imprint smears were hypercellular with the presence of numerous bare nuclei, which were predominantly lymphoid cells with a few plasmacytoid cells (Fig. 1). The bone marrow biopsy revealed a hypercellular marrow with diffuse infiltration of a spectrum of lymphoid cells that were predominantly small lymphocytes, plasmacytoid lymphocytes, a few plasma cells, and mast cells (Fig. 2). The erythroid, myeloid, and megakaryocytic series were markedly suppressed. Therefore, a diagnosis of lymphoplasmacytic lymphoma was considered. Immunohistochemical staining revealed 2 populations of cells; the predominant population was strongly positive for CD20 (lymphocytic cells) (Fig. 2 inset) while the other population was positive for CD138 (plasmacytic cells). CD5 and CD23 were negative, which ruled out chronic lymphocytic leukemia/small lymphocytic lymphoma. The serum protein electrophoresis revealed the following: total protein, 10.5 g/dL (range, 6.4-8.1); albumin, 1.76 g/dL (range, 3.50-5.64); gamma globulin, 7.18 g/dL (range, 0.62-1.53); and albumin to globulin ratio, 0.2 (range, 0.9-2.0), with an M spike of 5.98 g/dL. Immunofixation electrophoresis revealed IgM kappa light chains. Thus, a final diagnosis of WM was established.
DISCUSSION
A Swedish physician named Waldenstrom first described WM in 1944. WM, also known as LPL, is one of the rare subtypes of non-Hodgkin's Lymphoma (NHL), accounting for only 1-2% of all NHL cases [7, 8].
WM is defined as LPL with bone marrow involvement and an IgM monoclonal gammopathy of any concentration, and it is found in a significant proportion of patients with LPL [1].
WM occurs in adults with a median age between 60 and 70 years. Common presentation includes weakness and fatigue with an IgM serum paraprotein. The complications of LPL/WM include serum hyperviscosity, cryoglobulinemia, bleeding diathesis, amyloidosis, and pancytopenia; and these are related to the presence of increased levels of serum IgM and to tissue infiltration by lymphoplasmacytic lymphoma [1, 9-12].
Initially, it was believed that the skeletal system was not affected by WM. Moreover, absence of bone involvement in WM was considered a differentiating feature from multiple myeloma. Several subsequent reports indicated that skeletal involvement might be more common than previously believed [3-6]. Ju et al. [13] reported a case of a patient with WM, aged 50 years, who presented with a compression fracture of the spine . In multiple myeloma, plasma cells produce a monoclonal immunoglobulin as well as an osteoclast activating factor (OAF), which is a calcium mobilizing substance. OAF stimulates osteoclasts and therefore local bone resorption around the foci of myeloma while inhibiting local osteoblastic activity, leading to increased serum calcium levels. Marks et al. [5] suggested that, despite the fact that the lytic bone involvement in WM resembles that of multiple myeloma, the serum calcium levels in WM were consistently normal, suggesting that OAF was not present. Moreover, it has been observed that lytic lesions in WM are more common when there is a predominance of plasmacytic morphology [5, 6]. However, this was not reflected in the present case where the cell population was comprised primarily of lymphoid cells.
Involvement of the gastrointestinal system in WM is also rare [14, 15]. In our case, the CT scan indicated a thickening of the rectal wall and the wall of the sigmoid colon, suggesting a possible involvement of WM. The patient passed away; therefore, a biopsy could not be performed to confirm it.
In the present case, a clinical diagnosis of multiple myeloma was considered due to lytic bone lesions, decreased serum albumin, and low albumin to globulin ratio. However, there were a number of findings indicating that WM would have been a more appropriate diagnosis. These included the high percentage of lymphoid cells on the bone marrow biopsy, with only a few plasmacytic cells, and the increase in mast cells, a feature commonly observed in WM. In addition, the immunohistochemistry indicated a strong positivity for CD20 with only focal staining for CD138 which is contrary to the strong diffuse staining for CD138 observed in multiple myeloma. Lastly, the consistently normal serum calcium levels, despite the presence of multiple lytic lesions in the bone, also favored WM.
 XML Download
XML Download