

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Airway management in patients with complex facial trauma is quite challenging due to anatomical distortion that causes difficult oral and nasal intubation. Therefore, it is necessary to seek alternative techniques to secure the airway before and after a surgical procedure1.
Commonly, the airway is secured through endotracheal intubation. However, in patients with complex facial trauma involving cervical spinal cord injury, skull base fracture with or without rhinorrhea, nasal anatomy distortion, or lack of anesthesiologist experience, it is not possible to perform endotracheal intubation. In addition, many of these patients require intermaxillary fixation (IMF) in order to maintain normal dental occlusion transoperatively, which does not allow the use of orotracheal intubation because of the need for transient dental occlusion123.
One common option is tracheostomy, which is suggested for patients with severe head trauma that require ventilatory support for a prolonged period of time or in patients with polytrauma that will undergo several consecutive surgeries. However, this alternative includes multiple risks such as tracheal stenosis, tracheoesophageal fistula, bleeding, wound infection, recurrent laryngeal nerve injury, and visible scar4.
Another valid option not so commonly used due to its need for surgical experience is submental derivation. Described in 1986 by Hernández Altemir2, it promotes the establishment of a permeable and safe airway in patients with severe facial skeleton fractures, mainly those presenting with mid-third facial injury. This method facilitates management of the surgical area and the IMF, which is of vital importance for bone reconstruction45.
Submental derivation is an ideal alternative because it is a simple procedure that has the same advantages of nasal or orotracheal intubation to perform intraoperative IMF. It also allows the management of concomitant nasal or nasoorbitoethmoidal fractures1.
The contraindications of this procedure are that the patient refuses treatment, hemorrhagic diathesis, laryngotracheal disruption, surgical site infection, gunshot wound of the maxillofacial area, the need for prolonged mechanic ventilation, tumor ablation in the maxillofacial region, or past history of keloid scarring6.
The submental derivation procedure has its complications during the intraoperative time, such as sublingual and submental gland injury with its required ducts and lingual nerve injury. In the postoperative period, edema, obstruction, hematoma, lower airway infection, mucocutaneous fistula, and mucocele can develop78.
This study presents our experience in the use of submental derivation as a valid alternative for airway management in patients with complex facial trauma.
The study was approved by the Health Research Committee and Research Ethics of ISSEMyM Medical Center (approval no. 203F 39101/1000/CMI/51/2018), and informed consent was obtained.
Go to : 
II. Materials and Methods
This is a descriptive, retrospective study based on a review of medical records of all patients with facial trauma from January 2003 to May 2015. We included patients with midface Le Fort fractures I, II, and III and nasoorbitoethmoidal fractures in which intubation by submental derivation was indicated (impossibility for nasotracheal or orotracheal intubation and need for transient dental occlusion), regardless of age, sex, or trauma mechanism.
We followed a specific sequence to avoid complications and to make the process easily reproducible through identified critical steps.(Table 1) Prior intubation and, for patient and airway security, releasing the connector of the endotracheal tube is necessary in order to avoid further complications.
Table 1
Relevant steps for submental intubation
![]()
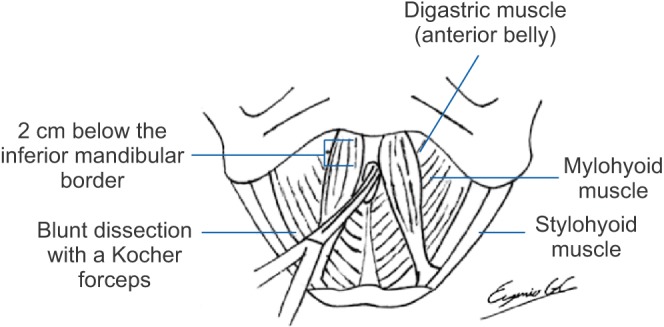
The anesthesiology team started the orotracheal intubation with an armed endotracheal tube according to patient measurements. Once the airway was secured, the patient was sterilely prepped and draped in the usual fashion. We proceeded corto mark a 1.5 cm horizontal line 2 cm below the inferior mandibular border. Then, we administered 2% lidocaine with epinephrine in the symphysis region.(Fig. 1)

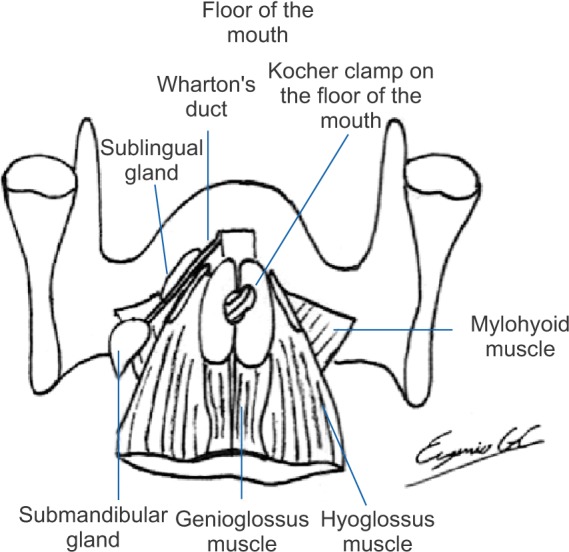
An incision was made only on the skin over the previously marked line, and blunt dissection was performed with Kocher forceps in a caudal-cephalic fashion over the midline close to the mandibular symphysis, through the subcutaneous tissue, while maintaining the dissection at the midline and avoiding the mylohyoid muscles and the anterior belly of the digastric muscle.(Fig. 2, 3) We continued all the way though the geniohyoid muscles and anterior to the submandibular glands and Wharton's duct, to finally disrupt the lingual vestibular mucosa and to observe the forceps through the mucosa of the floor of the mouth.(Fig. 4, 5)


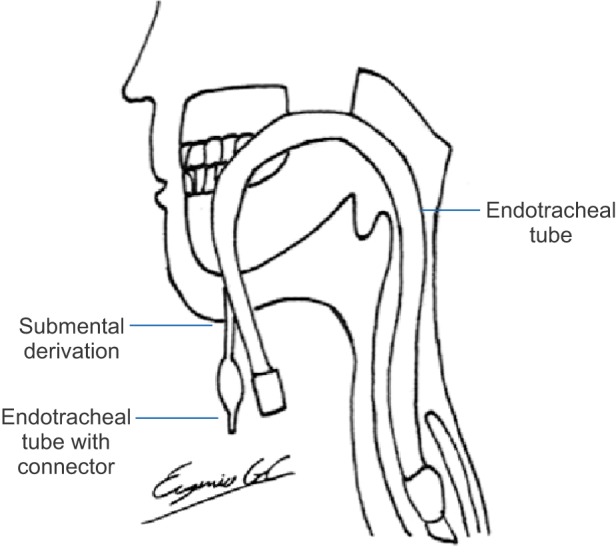
Once the tunnel is created, the previously released orotracheal tube connector is removed, and the tube is packed with sterile gauze to prevent the entrance of any fluid. The balloon insufflator is first applied with a clamp, and smooth traction is performed through the dissection toward the submandibular area. Then, the same procedure is performed with the distal end of the tube, while always manually securing the tube in its proximal portion.(Fig. 6) The gauze packing is removed, and the connector is placed (Fig. 7); confirmation of the correct endotracheal tube position is made by capnography and bilateral auscultation of lung fields. Fixation with #0 silk is done to join the tube to the ventilation system. It is then fixed with the same suture to the skin, hemostasis is verified, and the procedure is finished.(Fig. 8)


At the end of the surgery, the connector is once again removed, and the proximal portion of the tube is stabilized. The tube is moved in a retrograde manner to the oral cavity, and the globe is passed through it.
The subcutaneous tissue is closed with Vicryl 4-0 inverted knots, and the skin is closed with Nylon 5-0. Secondary healing closes the intraoral wound.
We performed this procedure in a systematic fashion, following the steps mentioned in Table 1.
Go to :
III. Results
None of the 31 patients included in this study developed any of the intraoperative complications secondary to this procedure as described in the literature4, nor in the immediate postoperative period or during the outpatient follow-up period.
The age range of the 31 patients was 14 to 71 years (mean age, 35.5 years); 27 patients were men, while four were women.
The trauma mechanism in most cases was car accident or gunshot. With regard to type, 78% were closed trauma, and the remaining 22% were open trauma. Fracture management was realized in all cases with IMF and open reduction and internal fixation with osteosynthesis material, with an mean time between trauma occurrence and surgery of 4.26 days (range, 1–20 days).
Of the 31 patients, 16 patients had a Le Fort fracture type I, 11 patients had a Le Fort fracture type II, three patients had a Le Fort fracture type III, and one patient had a nasoorbitoethmoidal fracture. The concomitant injuries are shown in Table 2.
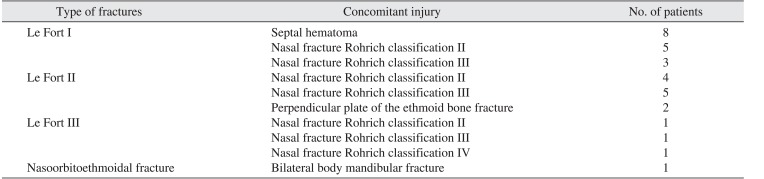
Table 2
Distribution of concomitant lesions
![]()
Go to :
IV. Discussion
Airway management in patients with maxillofacial trauma is difficult due to concomitant injuries. The normal anatomy distortion complicates endotracheal intubation, laryngoscopy, and the insertion of oropharyngeal cannulas. It is also indispensable in cases involving fracture of the mid-third of the facial skeleton to maintain the patients in normal occlusion and to perform internal fixation. The use of submental derivation has allowed the securement of a permeable airway in an easy and effective way9101112.
Submental derivation was described by Hernández Altemir2 in 1986 as an alternative to tracheostomy in patients with facial trauma5. MacInnis and Baig10 in 1999 described the incision in an inferior direction between the genioglossus muscle, the geniohyoid muscle, and the anterior belly of the digastric muscle. They also proposed their indication criteria: (1) minimum neurological deficit, (2) traumatic craniomaxillofacial injury, (3) need for intraoperative IMF for a short period of time to perform fracture reduction and fixation, (4) large pharyngeal flaps, and (5) rhinoplasty and craniomaxillofacial surgery13.
This type of airway management also avoids injury to nasal structures and the risk of cranial disruption with insertion of a tube into the cranial cavity, allowing manipulation of bone segments and tracheostomy exclusion. It is the preferred method of airway control in patients with maxillofacial fractures that do not require endotracheal intubation for more than 48 hours and patients in which nasotracheal intubation is not feasible4. A common alternative is tracheostomy, which requires a major surgical dissection and manipulation of important anatomical structures, as well as greater surgical time. Recurrent laryngeal nerve injury, thyroid gland injury hemorrhage, and tracheoesophageal fistulas are avoided9.
Patients with Le Fort II and III fractures, which involve the crib-shaped plate, have greater risks during nasotracheal intubation, such as cranial intubation, epistaxis, pharynx injury, nostril necrosis, otitis media, sinusitis, sepsis, and the impossibility to move the tube through the nose114. Orotracheal intubation does not allow the reduction and stabilization of the maxilla and mandible1. The advantages reported with submental derivation include: (1) avoidance of inherent complications of nasotracheal intubation and tracheostomy, (2) a simple procedure with low morbidity, (3) does not interfere with intraoral manipulation and maxillomandibular fixation, (4) can be used in patients with elective orthognathic surgery and patients with nasal obstruction such as cleft lip and palate patients, and (5) allows manipulation and treatment of the entire facial complex, with immediate withdrawal of IMF after the treatment is finished4.
Nonetheless, there exist potential complications of submental derivation such as superficial infection, mucocutaneous fistula, mucocele, sublingual and submaxillary gland and duct injury, and lingual nerve injury. Meyer et al.15 reported an 8% occurrence of oral floor abscesses and a 4% incidence of hypertrophic scar formation in a sample size of 25 patients16. However, none of these complications were presented in the 31 patients in which submental derivation was used through a midline approach. This demonstrates that, if the technique is performed meticulously and following the essential steps as described in Table 1, complications can be avoided, allowing appropriate IMF and a better approach for the treatment of complex facial fractures. Any surgeon could easily and safely perform this technique without expecting the same major complications that are currently associated with tracheostomy.
Go to :
V. Conclusion
If the relevant steps in the sequence proposed by our experiments are followed, the use of submental intubation is a safe and effective alternative for airway management in patients with facial trauma and concomitant injuries that do not allow the use of nasotracheal or orotracheal intubation. This method also avoids tracheostomy and its inherent complications. The performance of this technique could easily and safely be done by any surgeon following the described steps and sequence.
Go to :
 XML Download
XML Download