

 PDF
PDF Citation
Citation Print
Print



I. Introduction
Lipoma, a soft tissue lesion, is a benign tumour composed of mature adipose tissue. It is a common mesenchymal neoplasm that usually develops on the torso or proximal segments of the limbs1. Oral lipoma is rare, having an incidence of 1% to 5% among benign oral tumors2 and 0.3% among tongue neoplasias3. The most common sites are the buccal mucosa, lips, tongue, palate, vestibule, floor of the mouth, and retromolar area4. In 2004, Furlong et al.5 classified oral peripheral mesenchymal tumours as:
Clinically, they are all well-circumscribed, painless, slow-growing tumours. Their aetiology and pathogenesis are unclear, although factors such as mechanical, endocrine, or inflammatory issues2678; hypercholesterolemia; obesity910; radiation9; and chromosomal abnormalities1112 have been considered. Contributing risk factors include trauma, mucosal infections, and chronic or hormonal irritation. Lipoma usually affects male and female adults equally, and the most frequent age group is 40 to 50 years13. The lesions are slow-growing and often without symptoms; they are typically yellow in colour with a soft doughy consistency. A continuous increase in volume can interfere with phonation and mastication14. Lipomas usually occur as solitary lesions; multiple lesions can be associated with Gardner or Bourneville syndromes13.
II. Case Report
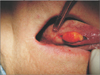
A 68-year-old Caucasian male presented with macroglossia that had developed from a slight swelling on the right lingual border, noted 3 years earlier. The neoplasm, involving the lateral edge of the ventral surface of the tongue, had a maximum diameter of 20 mm, a sinuous shape, and soft consistency. It was movable on the superficial and deep planes and covered by normal mucosa.(Fig. 1) It caused difficulty in swallowing and changes in sensitivity associated with occasional numbness on the tip of the tongue. His medical history did not reveal any systemic diseases. Palpation of the cervical lymph nodes and neck did not reveal any abnormality. To determine the places in which the patient experienced changes in sensitivity, the tongue was explored with a sharp pointed instrument. The patient reported hypesthesia and dysesthesia in the anterior third of the tongue. Oral magnetic resonance imaging with contrast medium confirmed the suspicion of lipoma. Fine-needle aspiration biopsy was performed, and the histopathology report indicated a predominance of mature adipose tissue with associated spindle cells embedded in myxoid stroma. No pleomorphic lipoblasts or areas of mitosis were observed.
The neoplasm was removed by transoral surgery.(Fig. 2) Local anaesthesia with articaine 1:100,000 (3.8 mL) was administered, a strip on the lingual border was marked, and the neoplasm was enucleated following the cleavage plane. The edge of the tongue was then sutured with silk size 3-0.
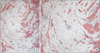
Macroscopic examination of the surgical material showed a capsulated mass, soft and yellowish in colour. It was placed in 10% buffered formalin and sent to the pathologist. Histological examination showed a well-circumscribed mass composed of lobules of mature adipose tissue and nodules of entrapped, non-neoplastic acini and ducts separated by thin, fibrous septa, compatible with lipoma.(Fig. 3)
The patient was given instructions for post-surgical care and pharmacological treatment. Antibiotics (amoxicillin and clavulanic acid twice daily for 5 consecutive days) and a corticosteroid (16 mg methylprednisolone for 3 days, then 8 mg for 3 days) were prescribed as well as chlorhexidine 0.2% anti-discoloration system mouthwash (three times a day after regular oral hygiene). Seven days after enucleation of the lesion, the sutures were removed. The surgical wound healed well, but dysesthesia on the top surface of the tongue persisted. The patient returned for weekly follow-ups and showed full neurological recovery 3 months after the operation.
III. Discussion
In 1848, Roux described lipoma for the first time as “yellow epulis”1. Lipoma is a common tumour of soft tissues and consists of mature fat cells arranged in lobules separated by layers of fibrous connective tissue. Although morphologically indistinguishable from normal fat, lipomas differ because their lipid is not available for metabolism, and they are usually surrounded by a thin fibrous capsule3. Lipoma is rare in the oral mucosa; 50% of oral lipomas occur in the buccal mucosa or on the tongue; less common areas are the floor of the mouth and lips2.
Lipomas in the oral mucosa might not be true tumours, but rather herniations of the buccal fat pad through the buccinator muscle. Such cases could occur as a result of local trauma in young children or surgical removal of third molars in older patients1. They manifest as soft and compressible masses of doughy consistency that are well defined clinically, radiologically (computed tomography), ultrasonographically, and by magnetic resonance imaging15. Other lesions that should be considered in differential diagnosis include oral lymphoepithelial, epidermoid and oral dermoid cysts, and connective tissue lesions such as granular cell tumours, neurofibromas, traumatic fibromas, and salivary gland lesions2. In the present case, a diagnosis of lipoma was confirmed by fine-needle aspiration biopsy. With regard to changes in sensitivity, the patient's medical history was negative for other surgery. The discomfort suffered was related to nerve damage caused by compression. Compression of the nerve trunk was found without damage to the axon, and this led to compression anaesthesia. Compression of the nerve axon led to dysesthesia that resolved after removal of the neoplasm. The slow growth of the lipoma probably initially deviated the lingual nerve from its regular path, and the subsequent compression caused dysesthesia. Lack of sensitivity in the tongue impedes phonation, mastication, and swallowing. It is worth remembering that biting the tongue can cause severe laceration and mutilation. Damage to the lingual nerve, as documented in the international literature, can occur during wisdom tooth extraction or other oral surgery. In the present case, the lesion was attributed to neuropraxia with no damage to the nerve trunk, as described by Seddon16. Complete surgical excision of the tumour can maintain adjacent structures but must include a rim of healthy tissue to prevent local recurrence17.

 XML Download
XML Download