

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
A recent literature review indicated that major aspects of the sagittal split ramus osteotomy (SSRO) design technique were in place with Hunsuck's modification of the basic Obwegeser-Dal Pont technique12. Subsequent modifications have generally focused on the attempts to manage or minimize the intra- or postsurgical problems that have since emerged123456.
The application of stable internal fixation systems has improved the predictability of orthognathic surgery and is an improved approach, especially compared with the osteosynthesis method, which only uses steel wire7. Some investigations have focused on internal fixation techniques; however, there is not currently a consensus, and many techniques do not have precise indications. Fixation plates should generally conform to the cortical bone to prevent disruption fragment alignments, which might induce undesirable changes in dental occlusion or in the condyle-fossa relationship. The locking plates/screw systems that have been used routinely prevent segment displacement even when the fixation plate is not in full contact with the cortical bone. In this system, the bone segments are not compressed against the plate or the screws89.
Most mechanical analyses have assessed the different types of osteosynthesis, but have not examined the effect of the SSRO design on the mechanical response. The osteotomy design can change the mechanical resistance, and the linear SSRO currently offers the best mechanical resistance10. Some modifications to the SSRO design have been made based on anatomical needs or to improve the results of the procedure. However, no adequate mechanical analyses have been conducted to examine differences among these approaches. The purpose of this study was to compare the mechanical resistance of four different osteosynthesis configurations in two different SSRO designs when subjected to linear loading.
II. Materials and Methods
A total of 40 synthetic polyurethane hemimandibles (Nacional Ossos, São Paulo, Brazil) were used in this research. Two polyurethane hemimandibles were sectioned in the ramus to simulate the two osteotomies designs using a reciprocating saw blade mounted in a hand piece; these models were replicated in a standard process. The hemimandibles were divided in two groups according to osteotomy design.(Fig. 1)
Group I: An osteotomy was performed 5 mm above the lingula by moving the reciprocating saw downward 14 mm. Then, a sagittal osteotomy through the lateral area of the second molar and between the two molars was performed so that the osteotomy descended perpendicularly to the basilar area.
Group II: An osteotomy was performed 5 mm above the lingula, moving the reciprocating saw downward 14 mm. Movement was then made sagittal to the distal edge of the second molar and then descended straight toward the anterior area, following the oblique line (lateral to the first molar), arriving at the basilar area of the mandible, with no angles created between the osteotomies.
Four subgroups (Fig. 2) were created, based on the internal fixation configuration, and each subgroup contained five hemimandibles.
A: One 4-hole 2.0 mm plate was fixed with four screws with a length of 5.0 mm;
B: One 4-hole 2.0 mm plate was fixed with four screws with a length of 5.0 mm and one bicortical screw with a length of 12.0 mm;
C: One 4-hole 2.0 mm locking plate was fixed with four screws with a length of 5.0 mm;
D: One 4-hole 2.0 mm locking plate was fixed with four screws with a length of 5.0 mm and one bicortical screw with a length of 12.0 mm.
To standardize the plate position, acrylic guides were made for each subgroup and adapted to the lateral aspect of the polyurethane hemimandibles during fixation of the plate. The samples were submitted to linear loading tests from the top to the bottom, in the first molar region, using the Instron (Instron 4411; Instron Corp., Norwood, MA, USA) machine. A metallic iron alloy support composed of a rectangular base and a vertical horn was constructed, giving the mandible rigidity and stabilization at three points of the posterior area of the condylar neck, mandibular ramus, and mandibular angle, avoiding clockwise rotation of the system during the linear load.(Fig. 3) The Instron 4411 produced linear displacement at a rate of 1 mm/min, and the loading was continuously applied up to failure of the internal fixation system.
The peak load and peak displacement were described and compared for statistical significance using one-way ANOVA in PASW Statistics 18.0 for Windows (IBM Co., Armonk, NY, USA). The Shapiro-Wilk test was performed, and the sample was found to be normally distributed. Levene's test was applied and showed homogeneity between the variances. Paired Student's t-tests were used to evaluate the average of the differences between the osteotomy designs for each internal fixation configuration (subgroup). The results were considered statistically significant at P<0.05.
III. Results
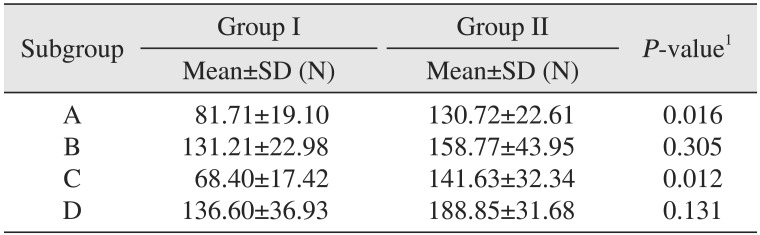
The SSRO design without right angles between the osteotomies (Group II) showed higher mechanical resistance than the SSRO design with right angles; however, the difference was not statistically significant. Table 1 shows the mean and standard deviation of peak load according to osteotomy design.
When the subgroups with the same internal fixation configuration and different osteotomy designs were compared, subgroups A (P=0.016) and C (P=0.012) showed a statistically significant difference (P<0.05). Table 2 shows the mean and standard deviation of peak load according to internal fixation system and osteotomy design.
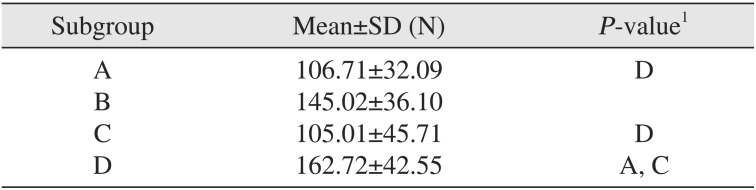
The subgroup peak loads were compared regardless of osteotomy design using one-way ANOVA; the results indicated that there was a statistically significant difference in peak load according to internal fixation system (F=5.26; P=0.004). A post-hoc Tukey test was performed, and the group with the 4-hole locking plate with one bicortical screw showed a significantly higher peak load (162.72 N) compared to subgroups A and C. Table 3 shows the mean and standard deviation of peak load according to internal fixation system regardless of osteotomy design.
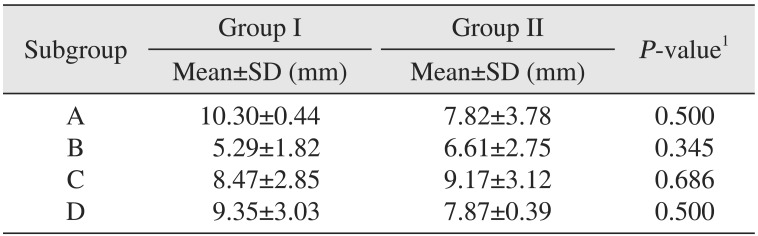
The peak displacement did not show normal distribution or heterogeneous variance; thus, a non-parametric analysis was performed. Group I showed a mean peak displacement of 10.30±0.44 mm, while Group II showed a value of 7.82±3.78 mm. There was no significant difference in peak displacement based on osteotomy design (Mann-Whitney U=172.5; P=0.457) or internal fixation configuration (Kruskal-Wallis χ2=6.55; P=0.08). Table 4 shows the results of peak displacement according to osteotomy design and internal fixation system configuration. The peak displacement of each subgroup was compared separately using the Wilcoxon test, and no statistically significant differences were found.
IV. Discussion
The osteotomy site stabilization technique after SSRO has improved since it was technically described by Trauner and Obwegeser11, and many fixation techniques are now available with predictable results regardless of osteotomy design. The osteotomy design has changed to reduce complications and facilitate improved techniques. However, the mechanism of how osteotomy design influences mechanical resistance has not been answered. This study found no differences in mechanical resistance related to osteotomy design when polyurethane hemimandibles were subjected to linear loading. However, when the mechanical resistance was evaluated according to internal fixation configuration and osteotomy design, the hybrid technique of one locking plate with one bicortical screw showed greater mechanical resistance.
In contrast to the results of this study, Pozzer et al.10 found that the SSRO designed with right angles between the osteotomies offered a higher peak load. The authors suggested that the angles present in the proximal segment of the SSRO may come into contact with the bone of the distal segment so that stress produces less resistance to the system and stimulates the torsional forces. However, these findings were reached at 3 mm of advancement of the osteotomy. At 7 mm of advancement, there was no statistically significant difference. Those authors used only one internal fixation system configuration, similar to subgroup A. In our study, we advanced the osteotomy by 5 mm, which could account for the different results.
The SSRO modifications were focused on attempts to manage or minimize the intra- or postsurgical problems, which included neurological injuries, unfavorable splits, relapse, fragment, and condylar resorption1. The stability and mechanical resistance of mandible segments and an internal fixation system depend on bone contact and plate and screw configurations; thus, the presence or absence of right angles between the osteotomies can have a minor impact on the mechanical behavior of SSRO. It is possible that the SSRO without right angles between the osteotomies could prevent stress concentration in areas and could minimize the risk of bad splits. However, it was observed that the subgroups fixed with one 2.0 locking and conventional plate showed differences in mechanical resistance related to osteotomy design, which could be due to the small sample size since the difference was not observed for all subgroups.
Analysis of the internal fixation configuration indicated that the subgroup with one locking plate with one bicortical screw showed higher mechanical resistance. Appropriate immobilization of the osteotomy segments ensures a simple healing process that guarantees favorable long-term results12. The introduction of the locking plate/screw system was an attempt to eliminate some of the disadvantages of conventional miniplates, such as screw loosening, need for precise plate adaptation to the bone, no bone segment traction to the plate, and avoidance of plate and screw compression against bone cortex, which could result in bone compression and local osteolysis813. Gutwald et al.13 verified in vitro that 2.0 mm locking plates show greater resistance than conventional plates and screws. Similar results have been reported by other authors14. The use of locking systems has been extensively proposed for use during treatment of facial fractures913, but their applications in orthognathic surgery deserve further attention1415.
Ribeiro-Junior et al.15 found that the locking screw/plate osteosynthesis systems had a slightly better performance in resisting bone displacement in mandibular sagittal osteotomy stabilization. However, this difference was not statistically significant. Our study did not identify statistically significant differences between the locking and standard systems when using hybrid techniques with one bicortical screw or between the one conventional and locking plate with monocortical screws. There were significant differences when the locking plate with one bicortical screws was compared to subgroups fixed with one conventional plate or one locking plate.
The use of a hybrid technique was initially proposed by Schwartz and Relle16, with the goal of incorporating advantages of the fixation with bicortical screws and miniplates with monocortical screws. This approach was based on two main arguments: improvement of mechanical resistance compared to fixation with miniplates and monocortical screws and facilitation of the fixation technique. From a mechanical perspective, a screw applied bicortically in the retromolar region inhibits segment displacement through its resistance to axial and shear stresses1718.
This present study had some limitations that are inherent to all in vitro investigations. It is not possible to compare the extent of static loading evaluated in this mechanical study with cyclical loading of chewing or biting. Changes in the loading point and the degree of SSRO advancement could alter the results. However, we chose to evaluate the area of the ipsilateral first molar because it produces a greater postoperative bite force than the incisive region. Unilateral molar change seems to generate the highest fracture-callus strain and exhibits the largest muscle recruitment activity. The mechanical advantages of the locking system and the use of a hybrid technique may not necessarily be reflected in better clinical outcomes, because the bone repair and stability of orthognathic surgery depend on several factors such as condylar displacement, direction of surgical movement, stretching of the suprahyoid muscles, posterior facial height increase, and multiple surgical segments.
V. Conclusion
Based on the results of this study, bicortical screw placement in the distal region promoted a better stabilization of SSRO. The osteotomy design was not associated with SSRO mechanical behavior influences when the hybrid technique was applied. Finally, the osteotomy without right angles offered higher mechanical resistance when one conventional or locking 2.0 mm plate was used.




 XML Download
XML Download