

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Open reduction and internal rigid fixation have been widely used for midfacial fractures1. Using these methods, the functional and aesthetic aspects of the oral and maxillofacial area can be restored. In some cases, however, unpredictable complications, such as malunion, paresthesia, facial deformities, and malocclusion, can occur23.
Among such complications, one of the most serious is malocclusion, because the first goal of open reduction surgery for maxillofacial fracture is restoration of the occlusion to its position before the injury. Postoperative malocclusion can be prevented only by proper alignment of the fracture segment based on sufficient consideration of the occlusion of the jaws4.
This a case report about malocclusion that resulted from lack of consideration for the occlusion when treating a patient with a midfacial complex fracture.
II. Case Report
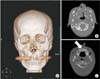
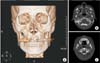
A 30-year-old man visited the emergency room with the complaint of a maxillofacial fracture due to a traffic accident that occurred nine days earlier in another country. At that time, he had received only first aid treatment consisting of primary sutures and removal of the glass fragments from the orbital area. He was transferred to the Department of Plastic Surgery. After clinical examination and radiologic studies, a Le Fort I plus II fracture was diagnosed, including fractures of the frontal bone, both inferior and medial orbital walls, nasal bone, hard palate, and multiple maxillary walls.(Fig. 1) Additionally, malocclusion including an anterior open bite and diastema due to the injury were detected.(Fig. 2) There was no consultation with the Department of Dentistry regarding the malocclusion.
The surgery was performed by plastic surgeons. Using a subciliary approach, both inferior orbital rims were reduced and fixed with absorbable plates and screws, and an absorbable mesh plate was placed into the left orbital floor after herniated inferior rectus muscle and fat were repositioned. Through the maxillary vestibular approach, the anterior maxillary wall was reduced and fixed with absorbable plates and screws. Then, closed reduction of the nasal bone was performed.(Fig. 3) Six days after surgery, the patient was discharged from the hospital; however, the day after discharge, he visited the outpatient clinic at the Department of Oral and Maxillofacial Surgery with a chief complaint of a malocclusion. The patient stated that he had had a close occlusion with well-aligned anterior teeth before the injury. On clinical examination, a generalized open bite tendency was detected. Only the right maxillary central incisor and the left maxillary second molar occluded with the opposing teeth. Additionally, a fracture of the root of the right maxillary lateral incisor, diastema, and mobility of right maxillary alveolar bone were also observed. Radiologic studies revealed vertical shortening of the maxilla.(Fig. 4) Thus, we recommended revision surgery for proper alignment of the fracture segments and restoration of occlusion. However, the patient refused the surgery for personal reasons. Therefore, only periodic follow-up observation was performed.
III. Discussion
Without sufficient consideration for the original occlusion, malocclusion can occur as a complication after fracture surgery. Such cases necessitate revision surgery, orthodontic treatment, or prosthetic treatments. Thus, for effective fracture treatment, systematic preoperative examinations including occlusion are necessary, and careful operative procedures are required upon performing the reduction5. Reported herein is a case where malocclusion remained after surgery due to the absence of such processes.
To restore the midface to its previous state in terms of height, width, and projection before the injury, reconstruction of skeletal buttresses is essential6. Insufficient reconstruction of the buttresses can cause facial deformity, improper occlusion, and additional damage to teeth or neurovascular bundles. Among these, the postoperative alteration of the occlusion is one of the complications that commonly occur in surgery for fracture management. It mostly occurs when the occlusal relationship before the injury is ignored in the operating room. The occlusion before the injury must be reproduced using intermaxillary fixation (IMF), and IMF must be stable during the fixation procedure. Additionally, to avoid forcible IMF, it is recommended that IMF be performed after the fracture line is exposed. Using this maneuver, surgeons can simultaneously ensure appropriate alignment of the fracture line and proper occlusion7. In the present case, since proper restoration of the midface buttress and IMF were not performed, the correct rearrangement of the maxilla failed, and the malocclusion persisted after the surgery.
Maxillary arch fractures occasionally involve fractures of the alveolar bone and median palate, which frequently occur before 30 years of age. The treatment goals of these fractures include reconstruction of a stable and adequate maxillary arch width, correct arrangement of the teeth, and placement of proper inclination to the alveolar bone8. For palatal fractures, the complication of malocclusion can be minimized using a simple and effective palatal splint during the open reduction and internal fixation procedure9. In the present case, the diastema persisted due to insufficient reduction of the anterior palatal suture. As jaw fractures are often accompanied by dislocation of teeth, fixation of the tooth itself, such as by resin-wire splinting, is required10. With this case, however, consideration of this issue was also not sufficient; as a result, the positions of the teeth were unstable.
A revision was necessary due to the malocclusion caused by an improper fracture reduction. However, reoperation is usually a heavy burden to the patient. To prevent this serious complication and revision surgery, it is important to gain insight about the original occlusion through an accurate preoperative diagnosis. In the operating room, surgeons should also restore the original buttress and perform rigid fixation using IMF and a prefabricated palatal splint as needed.


 XML Download
XML Download