

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Acquired immunodeficiency syndrome (AIDS) is the disease of the immune system triggered by infection with human immunodeficiency virus (HIV). The virus will gradually destroy the immune system, which makes it difficult for the body to fight infections1. This leaves the patient vulnerable to opportunistic infections2. HIV/AIDS constitutes a worldwide pandemic12.
In 2015, approximately 36.7 million people (34.0-39.8 million people) had HIV worldwide, and 2.1 million people(1.8-2.4 million people) became newly infected with HIV. As of December 2015, 17 million people living with HIV were accessing antiretroviral therapy. In 2015, 1.1 million people (0.94-1.3 million people) died from AIDS3.
The late expression of HIV infection is characterized by state of complete immunodeficiency, caused by diminished CD4+ (cluster of differentiation 4) cells4. Thus, the CD4+ cell level serves as a marker of disease progression45. Within the evolution of disease, the CD4+ cell count generally decreases about 30%, whereas the CD8+ (cluster of differentiation 8) cell count may increase about 40%. This results in an inverted CD4+/CD8+ cell ratio that is usually less than 1 (while the normal ratio may vary between 0.9 and 3.7)67.
There are 40 known oral lesions of AIDS according to the European Economic Community57. There are two main classification systems for these oral lesions associated with HIV (HIV-OL). The first is based on the HIV-OL etiology: lesions are classified as bacterial, viral, fungal, neoplastic, or other. In 1993, the EC-Clearinghouse on Oral Problems Related to HIV Infection and the WHO Collaborating Centre on Oral Manifestations of the Immunodeficiency Virus reached consensus on a new classification system for the oral manifestations of HIV infection. This system classifies HIV-OLs into three groups: lesions strongly associated with HIV infection, lesions less commonly associated with HIV infection, and lesions seen in HIV infection6. Oral lesions may be associated with acute pain, incompetence to swallow, and difficulty in eating. They may also compromise facial appearance. In immune-compromised patients, Candida species can generate a variety of oral lesions ranging from localized to disseminated candidiasis89. Oral candidiasis is the most frequent feature of AIDS in the mouth, with a prevalence of 70% to 90%8910. Hairy leukoplakia, non-Hodgkin's lymphoma, and Kaposi's sarcoma have a wide association with HIV infection and are labeled as AIDS-defining conditions111213. In some cases, enlargement of the parotid glands and adenopathy can be observed during head and neck examination of HIV-infected patients131415.
Aside from their diagnostic importance, oral lesions may be of prognostic importance for the development of AIDS. They can serve as clinical correlates with CD4+ and CD8+ cell counts161718. CD4+ T-cells are the main target of HIV; their diminution severely limits a patient's immune capacity19. When the CD4+ lymphocyte count decreases to a point where new CD4+ cell production is insufficient, the immune system yields to the clinical manifestation of AIDS42021. While measuring CD4+ and CD8+ cell counts requires a laboratory blood analysis, the identification of oral lesions can be done during physical examination.
The aim of this study was to evaluate the oral lesions of 75 HIV/AIDS patients, in order to assess their correlation with CD4+ cell counts (including the CD4+/CD8+ cell ratio).
Go to : 
II. Materials and Methods
A total of 75 patients with HIV/AIDS were assessed in a descriptive, cross-sectional study spanning two years. Relationships between oral lesions, CD4+ and CD8+ cell counts, and the CD4+/CD8+ cell ratio were investigated. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Ethical Committee of Saint-Antoine Hospital was obtained (no. 94REIM0201), and informed consent was obtained from all individual participants included in the study.
Patient records from the Odontology Unit of Saint-Antoine Hospital were initially checked, and selected patients were asked to visit the unit for further examination. Each patient's medical history was noted, and a physical examination of the head and neck area and oral cavity was performed. The medical record, physical examination, demographic data, and laboratory tests were then assessed. Based on the findings of the physical inspection and laboratory tests, patients were prescribed essential medication, and follow-up visits were considered.
One qualified practitioner carried out all oral examinations. Extra-oral and intra-oral areas were examined first, followed by intra-oral tissues removed for pathology. Biopsies were taken for histological diagnosis only when needed. The assessment of oral lesions was implemented using the EC-Clearinghouse guidelines established in conjunction with the World Health Organization in 19936. When multiple lesions were observed in the same patient, each lesion was considered independently for analysis.
Candida colonization was identified by isolation of Candida species from the oral cavity. A single oral swab was collected from each study participant. Swabs were cultured on Sabouraud's dextrose agar with chloramphenicol (0.5 g/L). Plates were incubated at 37℃ in aerobic conditions and observed daily for one week.
CD4+ and CD8+ cell counts were also analyzed. Based on the World Health Organization classification system for immunodeficiency3, patients with CD4+ cell counts >500 cells/mm3 were classified as “marginally” immunodeficient; patients with CD4+ cell counts 200-500 cells/mm3 were classified as “mildly” immunodeficient; and patients with CD4+ cell counts <200 cells/mm3 were classified as “severely” immunodeficient. Collected data were analyzed using the SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA). Statistical variables included patient demographics (social demographics, age, and gender), types of oral lesions present, the amount of CD4+ cells, and the CD4+/CD8+ cell ratio.
Go to :
III. Results
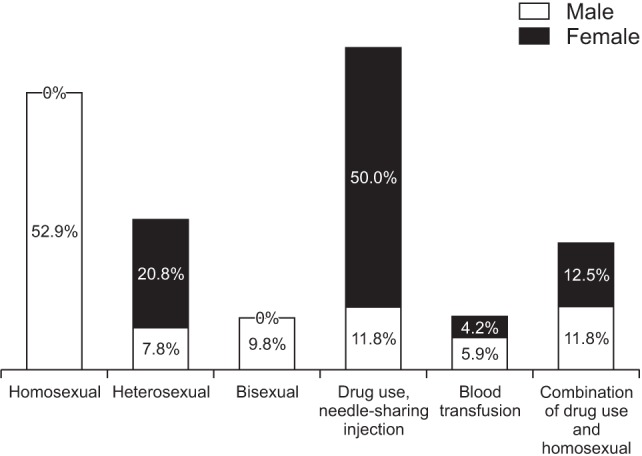
Of the 75 patients, 51 patients (68.0%) were males and 24 patients (32.0%) were females. The median age in this study group was 38 years (range, 22-54 years). Of the patients, 44 patients had a history of sexual exposure to HIV, 18 patients had a history of sharing intravenous needles, 9 patients had a history of both sexual exposure and sharing intravenous needles, and 4 patients had a history of blood transfusion.(Fig. 1)
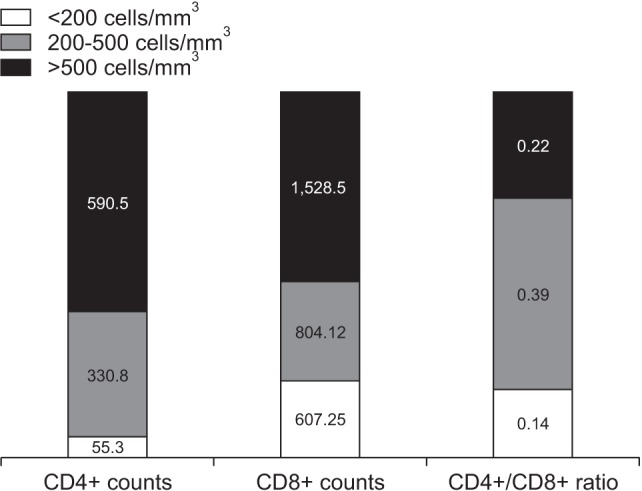
The CD4+ count was <200 cells/mm3 in 45 cases, 200-500 cells/mm3 in 18 cases, and >500 cells/mm3 in 12 cases. The mean CD4+ cell count was 158.75 cells/mm3 in males and 144.50 cells/mm3 in females.(Fig. 2) The median duration of antiretroviral therapy-mediated viral suppression was 3 years (range, 3 months to 4 years).
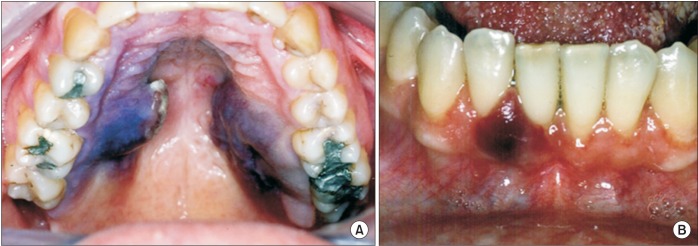
The distribution of oral lesions and the CD4+ cell counts of HIV-infected patients are shown in Fig. 3. All patients showed at least one oral manifestation. The most common oral lesion identified was oral pseudomembranous candidiasis (OPC, accounting for 80.0%), followed by periodontal disease (PD, 40.0%), herpetic lesions (HL, 16.0%), hairy leukoplakia (HLP, 16.0%), gingivitis (G, 20.0%), oral ulceration (OU, 12.0%), Kaposi's sarcoma (KS, 8.0%), and non-Hodgkin's lymphoma (NHL, 4.0%).(Fig. 4,5,6,7)
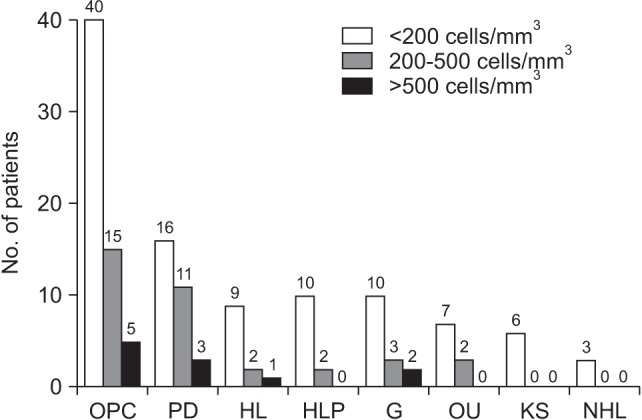 | Fig. 3Distribution of oral lesions and CD4+ cell counts. (OPC: oral pseudomembranous candidiasis, PD: periodontal disease, HL: herpetic lesions, HLP: hairy leukoplakia, G: gingivitis, OU: oral ulceration, KS: Kaposi's sarcoma, NHL: non-Hodgkin's lymphoma)
|
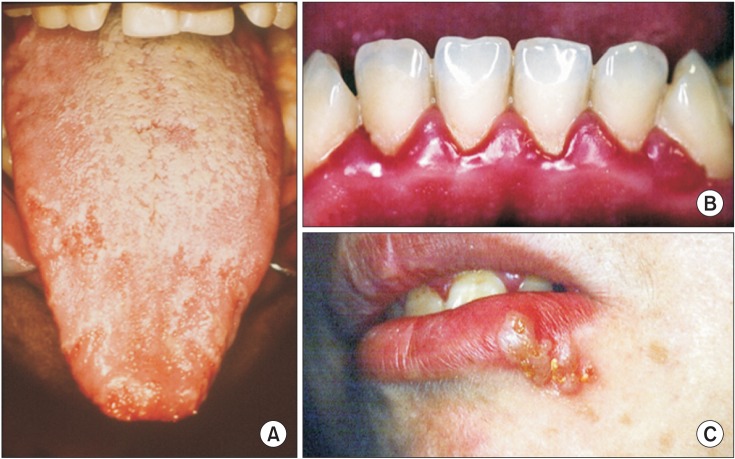 | Fig. 4Clinical appearance of oral lesions. A. Pseudomembranous candidiasis of the tongue. B. Swelling and redness of the gums as a clinical sign of periodontal disease. C. Herpetic lesion-type vesicles on the lower lip.
|
 | Fig. 5A. Hairy leukoplakia of the lateral border of the tongue. B. Ulcerous-necrotic material of the gums as a clinical sign of gingivitis. C. Ulcerations localized on the uvula and the lateral walls of the tonsils.
|

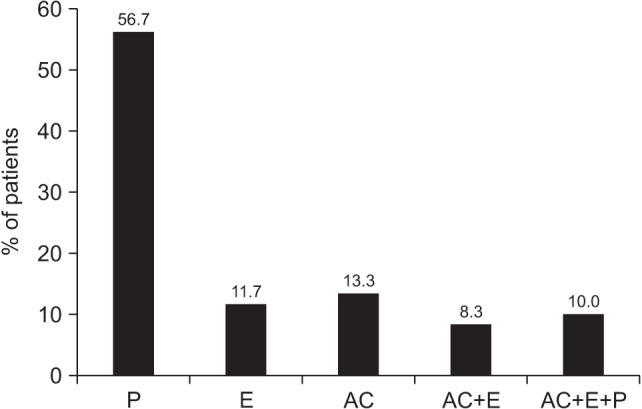
Five different clinical presentations of OPC were observed on examination. Pseudomembranous (P) OPC was the most common clinical presentation (34/60 cases), followed by erythematous (E) OPC (7/60 cases), angular cheilitis (AC) (8/60 cases), a combination of AC and E (5/60 cases), and a combination of AC, E, and P (6/60 cases).(Fig. 8) Candida albicans was the most frequent species isolated (82% of cases), Candida tropicalis was isolated in 10% of cases, and Candida glabrata was isolated in 8% of cases.
Go to :
IV. Discussion
Oral lesions are common findings in HIV-infected patients, and OPC is the most prevalent lesion type. The major reason for the development of oral lesions is the destruction of the immune system, and specifically the destruction of CD4+ lymphocytes18. CD8+ T-cells play a crucial role in controlling HIV replication during the early phase of infection. HIV-specific CD8+ T-cells are targeted toward the dominant viral variant, and their emergence is associated with a rapid fall in viral load before the development of an antibody response18.
HIV infection is characterized by a progressive decrease in the absolute number of circulating CD4+ cells and in the CD4+/CD8+ cell ratio. In this study, no correlation was found between the CD4+/CD8+ cell ratio and oral lesions. But a strong correlation was found between the CD4+ cell count and oral lesions. The explanation for these findings could be related to the anti-viral treatments given to patients. In untreated HIV infection, CD8+ cell counts increase as CD4+ cell counts decline22. During antiretroviral therapy, some individuals achieving CD4+ cell counts above 500 cells/mm3 experience a simultaneous decline in CD8+ cell counts, leading to a normal CD4+/CD8+ cell ratio. Among HIV-negative adults, inversion of the CD4+/CD8+ cell ratio (below 1.0) predicts all-cause mortality and is considered part of the immunogenicity phenotype2324252627. In the setting of untreated HIV infection, the CD4+/CD8+ cell ratio predicts progression to AIDS24.
In this study, the average age of the patients was 38 years, and males were predominant (68% vs 32%). Thus, a high level of HIV/AIDS was found among youthful patients. Sexual contact was the main route of HIV transmission (58.7% of cases), followed by shared intravenous needles (24.0%) and blood transfusions (5.3%). Infection of females was primarily through shared intravenous needles, while males were more commonly infected through sexual contact.
The most common oral lesion identified was OPC (accounting for 80.0% of cases, 60/75), followed by PD (40.0%, 30/75), HL (16.0%, 12/75), HLP (16.0%, 12/75), G (20.0%, 15/75), OU (12.0%, 9/75), KS (8.0%, 6/75), and NHL (4.0%, 3/75). Candida species were isolated from the oral cavity in 76% of cases. Similar figures have been recorded by Thompson et al.28, Castro et al.29, and Lin et al.30.
In our study, 60.0% of the oral lesions were in patients with CD4+ cell counts <200 cells/mm3. This is consistent with previous studies, in which HIV patients with CD4+ cell counts <200 cells/mm3 had more oral lesions161821.
An inverse correlation between CD4+ cell counts and the presence of oral mucosal lesions in HIV-infected patients has been reported8212526. Similarly, the present study has found a significant inverse correlation between CD4+ cell counts and the prevalence of oral lesions in HIV-infected patients. The distribution of OPC lesions according to CD4+ cell counts (73% of lesions were in patients with CD4+ cell counts <200 cells/mm3) has been a common observation in other studies as well19. This indicates that the occurrence of oral lesions in HIV patients could be helpful in determining immunological status. This finding also corresponds with reports that CD4+ cell reduction is strongly associated with a high viral load18. For these reasons, clinicians and physicians are regarding oral lesions as useful for the diagnosis and detection of infection progression1826.
The main factor associated with the development of oral opportunistic lesions is the CD4+ cell count20. The onset of oral candidiasis and oral hairy leukoplakia is indicated by a sustained reduction in the CD4+ blood cell count together with a sharp increase in viral load10. Moniaci et al.8 observed that oral lesions found among 737 persons infected with HIV in Italy were significantly associated with CD4+ cell counts <300 cells/mm3. In a study on 43 HIV-positive subjects in Greece, Kolokotronis et al.9 reported that oral hairy leukoplakia was associated with CD4+ cell counts <200 cells/mm3. And Adurogbangba et al.27, by analyzing oral lesions and CD4+ cell counts in 81 HIV-positive and 31 HIV-negative subjects in Nigeria, found that CD4+ cell counts <500 cells/mm3 were significantly associated with pseudomembranous candidiasis and angular cheilitis. Similarly, the present study has revealed that the presence of oral candidiasis and hairy leukoplakia are associated with CD4+ cell counts <200 cells/mm3.
The Centers for Disease Control and Prevention have proposed a revised classification system and AIDS case surveillance definition that incorporates both clinical signs and symptoms and one laboratory marker, the CD4+ cell count7. Thus far, the CD4+ cell count has been recognized and widely used as a marker for HIV-related disease progression. Conclusions from the present study indicate that the existence of oral lesions in HIV patients could be useful to monitor immunological status. Results from the present study are consistent with previous reports that CD4+ cell depletion is strongly associated with a high viral load18. The development of oral lesions caused by opportunistic pathogens is significantly related to the CD4+ cell count18. The onset of certain oral lesions (such as those in candidiasis and oral hairy leukoplakia) is signaled by a sustained reduction in the CD4+ blood cell count, which is associated with a high viral load11.
Go to :
V. Conclusion
As the CD4+ cell count decreases, the appearance and severity of oral lesions increases. A diagnosis of oral lesions may point to a positive HIV/AIDS status. Progression of infection is associated with a high prevalence of certain oral lesions, including candidiasis, hairy leukoplakia, and Kaposi's sarcoma. The severity of lesions is more pronounced with a low CD4+ cell count. Management of lesions will improve quality of life for HIV/AIDS patients. An awareness of the connection between oral lesions and disease progression is recommended for clinicians treating HIV infection.
Go to :
 XML Download
XML Download