

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Cavernous sinus thrombosis (CST) was first described by Bright in 1831 as a complication of epidural and subdural contamination1. As a result of its intricate neurovascular anatomic relationship, CST is the most complicated type of intracranial septic thrombosis2.
The occurrence of CST has always been low, with only approximately 200 case reports found in literature. Prior to the advent of efficacious antimicrobial agents, the mortality rate from CST was effectively 100%. Typically, death from CST is due to sepsis or central nervous system infection. With aggressive management, the mortality rate is presently less than 30%3. Although dental infections are not a common source of CST, they can cause sinusitis, orbital cellulitis, parapharyngeal abscess, mediastinitis, and pericarditis45. There are very few reports of CST identified with periodontal disease or tooth extraction6.
CST can result from infection of the paranasal sinus or any of the anatomic structures drained by the cavernous sinus, including the mid-face, orbit, and oral cavity7.
We present an unusual and rare case report of CST after dental extraction.
II. Case Report
A 40-year-old female patient reported to the emergency department of the medical school with swelling in the right side of the face over the previous 11 days. There was a history of extraction of an upper right back tooth 11 days prior by an unregistered dental practitioner. The patient was feeling normal until she noticed the swelling on the right side of her face, which gradually progressed to its present size. Pain was associated with the swelling and was continuous and dull in nature. The patient underwent removal of the upper right third molar by an unregistered dental practitioner in her village. After the procedure, the patient had continuously visited the practitioner with a complaint of pain and an unhealed socket in the right maxillary posterior region. Furthermore, she developed swelling on the right side of her face with decreased mouth opening. The patient was referred to the medical school by the unregistered dental practitioner. The patient's medical history did not reveal anything significant.
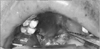
The patient's general condition was toxic with a Glasgow coma scale (GCS) score of 11 and a temperature of 40℃. Upon examination, the swelling was tender, fluctuant, and extended superior inferiorly from the temporal region to the inferior border of the mandible and anteroposteriorly from the angle of the mouth to the angle of the mandible along with necrosis over the right infraorbital region.(Fig. 1) The patient presented with diplopia, dilated pupil, proptosis, periorbital ecchymosis, loss of vision, abducens nerve palsy, and chemosis of the right eye.(Fig. 2) Intraorally, the maxillary tuberosity was fractured, and necrosis of the palatal mucosa and upper right vestibule was also present.(Fig. 3)
Blood examination revealed a random blood sugar value of 311 mg/dL, total leucocyte count of 18,200 cubic millimeter of blood, and polymorph value of 92%. A computed tomography (CT) scan revealed mucosal thickening involving the bilateral maxillary and right ethmoidal sinuses with venous dilatation of the right superior ophthalmic vein, suggestive of thrombosis.(Fig. 4) A CT scan of the face revealed an abscess in the right side of the buccal and temporal spaces.
Based on empirical therapy, the patient was immediately treated with intravenous antibiotics, including an injection of imipenem 500 mg intravenously every six hours, an injection of clindamycin 600 mg intravenously every 12 hours, an injection of ceftriaxone (Rocephin) 1 g intravenously every 12 hours, an injection of chloramphenicol 1 g intravenously every 8 hours, and an injection of metronidazole 500 mg intravenously every 8 hours for three consecutive days.
Other drugs included an injection of furosemide 10 mg/mL intravenously every 8 hours, an injection of mannitol 20% 100 mL intravenously every 8 hours, an injection of dexamethasone 8 mg intravenously every 8 hours, nonsteroidal anti-inflammatory drugs, and paracetamol for fever. An injection of human mixtard insulin 12 units subcutaneously every 12 hours and low molecular weight heparin 5,000 units subcutaneously every 12 hours were added along with antibiotic treatment. The above-mentioned drugs were given to the patient consecutively for three days.
On the basis of clinical and radiological features, a provisional diagnosis of CST was made. On the second day of hospitalization, the patient underwent emergency incision and drainage of the right buccal and temporal spaces under general anesthesia and was admitted to the intensive care unit. Several hours after surgery, the patient exhibited signs of chemosis in the left eye and paralysis of the contralateral side of the body. Her GCS score decreased to 7 with no signs of improvement. The patient was put on a ventilator under close observation of the emergency medicine department and continued the previous treatment with regular follow-up by a team of oral and maxillofacial surgeons.
Unfortunately, two days after the surgery, the patient died due to complications of the disease, which included meningitis, septic emboli, blindness, cranial nerve palsies, sepsis, and shock.
III. Discussion
The cavernous sinus is a dural venous sinus situated lateral to the sella turcica, between two layers of cranial dura, in the middle cranial fossa. Structures present within the cavernous sinus include the third, fourth, and sixth cranial nerves; ophthalmic and maxillary divisions of the fifth cranial nerve; and internal carotid artery with its surrounding sympathetic plexus.
The superior and inferior ophthalmic veins and sphenoid and middle cerebral veins empty into the inferior petrosal sinuses and then into the internal jugular veins and the sigmoid sinuses via the superior petrosal sinuses. Blood can flow in either direction, as these complex webs of veins are valveless. Facial infections involving the nose, tonsils, and orbits can easily spread by this complex pathway to the cavernous sinus.
According to Shaw8, various routes of infection that can lead to septic thrombosis are 1) from the face through the angular and ophthalmic veins, 2) from the middle ear through the superior petrous sinus, 3) from the teeth, maxillary sinus, and cervical vertebrae through the pterygoid plexus emptying into the inferior ophthalmic vein, 4) from the sphenoid sinus by direct extension or draining emissary veins, 5) by extension from an infected internal jugular vein, lateral sinus, or petrosal sinus, or 6) from the plexus of veins surrounding the internal carotid artery. The spread of infection in the presented case was likely from the pterygoid plexus to the inferior ophthalmic vein to the cavernous sinus.
CST is commonly associated with sphenoid and ethmoid sinus inflammation in comparison to frontal sinus inflammation. Uncontrolled diabetes mellitus patients have a greater risk of developing chronic sinusitis. Our patient was diagnosed with uncontrolled diabetes mellitus that could have been the cause of her CST.
Eagleton9 suggested six criteria for establishment of diagnosis: 1) a known site of infection, 2) an infection of the blood stream, 3) early signs of venous obstruction, 4) involvement of nerves in the sinus, 5) a neighborhood abscess of the soft parts, and 6) symptoms of complicating disease.
Evaluation for CST should be performed for patients presenting with headache and any cranial nerve abnormality. The typical signs and symptoms are related to cranial nerves present within the cavernous sinus. Focal cranial nerve abnormalities can be present in some cases of CST, possibly resembling an ischemic stroke10.
The earliest physical finding of CST can be periorbital edema, almost always accompanied by fever; both headache and periorbital pain worsen with time. Paresthesia in the distribution of the first and second trigeminal nerves can occur. Occlusion of the ophthalmic veins can lead to chemosis. The abducens nerve lies freely within the sinus, in contrast to cranial nerves III and IV, which lie within the lateral walls of the sinus. Therefore, lateral gaze palsy is usually seen first due to the involvement of cranial nerve VI11. Cranial nerve III dysfunction leads to mydriasis, ptosis, and weakness of the eye muscle. Similarly, the above-mentioned findings were present in our patient, including chemosis, involvement of the 3rd, 4th, and 6th cranial nerves, exophthalmos, and fixed pupil and periorbital edema of the right eye extending toward the left eye, which are pathognomonic of CST.
Connections are also present between the contra-lateral cavernous sinus, the intercavernous sinus, and facial veins that do not have a valve. The pterygoid plexus, which is located very close to the cavernous sinus, possesses bilateral orbital symptoms or symptoms on the opposite side12. Diplopia, dilated pupil, proptosis, periorbital ecchymosis, loss of vision, abducens nerve palsy, and chemosis of the right eye, which later spread to the opposite side, were present in our patient.
In the CT scan, CST can be visualized as an area of increased density. Exophthalmos, soft tissue edema, and dilation of the superior ophthalmic vein can also be visualized on CT scan.
Magnetic resonance imaging (MRI) is used to differentiate CST from orbital cellulitis, as they have similar clinical presentations and involvement of the parotid gland. Magnetic resonance venography shows the absence of venous flow in the affected cavernous sinus. Carotid angiography, MRI, and CT can visualize the narrowing and/or obstruction of the carotid artery.
Usually, patients with CST have leukocytosis. In support of this, in the presented case, the leucocyte count was 18,200 cubic millimeter of blood.
The treatment of CST includes the use of antibiotics directed at the causative organism and surgery to remove the primary source of infection. Immediate empirical antibiotic coverage must include gram-positive, gram-negative, and anaerobic bacteria. Further treatment can be narrowed and adjusted to cultures and sensitivities.
Maintaining the partial thromboplastin time or thrombin clot time at 1.5 to 2 times that of the control, intravenous heparin can be given at a dose greater than 24,000–30,000 U/day. Heparin counteracts the conversion of fibrinogen to fibrin and thus inhibits further thrombogenesis. To prevent the spread of thrombosis to the other cavernous sinus as well as to the inferior and superior petrosal sinuses, heparin should be introduced as early as possible. The use of heparin is disputable, as retrospective studies show conflicting data. The decision to use heparin should be based on thorough consultation with a specialist13.
In cases of pituitary insufficiency, corticosteroids are absolutely indicated as they help to lessen inflammation and edema and prevent residual cranial nerve dysfunction brought on by inflammation. In patients with Addisonian crisis secondary to ischemia or necrosis of the pituitary that convolutes CST, the use of corticosteroids is necessary.
Complications include intracranial extension of infection that can result in meningitis, encephalitis, brain abscess, pituitary infection, and epidural and subdural empyema. In addition, cortical vein thrombosis can lead to hemorrhagic infarction and extension to other sinuses.
In conclusion, CST is a rare disease, but the mortality rate remains high, even after the breakthrough of antibiotics and advanced imaging techniques. Unethical practices by unregistered practitioners and a lack of awareness of dental health in rural areas can lead to severe life threatening complications of dental infections, as seen in our case. Therefore, dental health education in rural areas, legal action against unregistered practitioners, early diagnosis, and aggressive antibiotic treatment can prevent future mortality because of CST.



 XML Download
XML Download