

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Although condylar fractures represent approximately one-third of mandible fractures, the treatment is still controversial. Treatment of condylar fractures can be roughly divided into closed reduction and maxillomandibular fixation (CRMMF) and open reduction and internal fixation (ORIF).
Surgical open reduction is determined depending on the displacement or dislocation of the fractured condylar head. In the presence of severe medial displacement, dislocation of a condylar fragment, or high condylar fracture, extracorporeal operation is considered for reduction and fixation of the condylar fragment under direct vision. However, in such cases, there is a greater possibility of postoperative condylar resorption such as with a free graft.
Thus, we did not remove the condylar and ramal fragments from the body after vertical ramal osteotomy. Reduction and fixation were performed in the intracorporeal state.
II. Cases Report
1. Surgical procedure
First, the Risdon incision was performed for the submandibular approach on the mandibular angle, and dissection was performed down to the mandibular border. At the time of dissection, the medial pterygoid muscle on the ramal bone was not detached in order to preserve the blood supply. With this procedure, prompt blood supply to osteotomized ramal bone will be ensured. Although the fracture line was exposed in the operation field, the lateral pterygoid muscle affected the antero-medial dislocation of the condylar fragment, which was blocked by the ramal part of the muscle. Therefore, a vertical ramus osteotomy was required to pull down the condylar fragment and perform internal fixation. After drawing the osteotomized line and temporary adaptation of the fixation plate, ramal vertical osteotomy with anterior extended design on the angular border area was performed.(Fig. 1) Then, after displacing the ramal fragments medially and detecting and pulling down the condylar fragment, this fragment was reduced to the posterior ramal part in the intracorporeal state, and internal fixation was performed with two 4-hole miniplates.
Reduced condylar and osteotomized ramal fragments were repositioned to the original ramal body and fixed with two preadapted miniplates.(Fig. 2)
The patient underwent intermaxillary fixation for one week after the operation and mouth movement exercise with elastic traction for another week.
2. Case 1
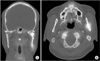
On March 30, 2014, a 43-year-old male patient visited our outpatient department with complaint of pain on the left side of the jaw after a fall. Clinical examinations showed pain on the left side of the jaw, occlusal change, and mouth opening limitation. On preoperative radiographs, a left condylar fragment was dislocated to the antero-medial position.(Fig. 3) This patient underwent open reduction through the technique described above. Postoperative radiographs showed good anatomical reduction of the condylar fragment in the glenoid fossa.(Fig. 4. A) There were no signs of mandibular condylar resorption until postoperative 3 weeks.(Fig. 4. B) Blood supply to the condylar and osteotomized ramal fragments were represented by hot spots on the left fragments on postoperative 1-week single photon emission computed tomography (SPECT).(Fig. 5)
3. Case 2
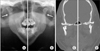
On June 14, 2014, a 25-year-old male patient visited our outpatient department via the emergency center. Clinical examinations showed pain on both side of the jaw, open bite, and mouth opening limitation. On preoperative radiographs, both condylar fragments were displaced to the medio-inferior position and overlapped the ramus.(Fig. 6) Postoperative radiographs showed good anatomical reduction of both condylar fragments in the glenoid fossa.(Fig. 7. A, 7. B) On postoperative 1-month radiographs, there were signs of displacement of both condylar fragments with right plate fracture and left screw loosening.(Fig. 7. C) However, the postoperative 4- to 6-month radiograph showed bone remodeling at the displaced fracture site with increased radiodensity. Finally, the postoperative 2-year radiograph showed complete remodeling of the condylar fragments with restored anatomic appearance.(Fig. 7 D) There were no signs or symptoms of mandibular condylar dysfunction during the healing and remodeling periods.
4. Case 3
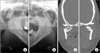
On January 16, 2016, a 39-year-old female patient visited our outpatient department via the emergency center. After receiving first-aid, she reported to our hospital with complaint of fractures on both sides of the jaw after a fall. Clinical examination showed occlusal change and mouth opening limitation. On preoperative radiographs, both condylar fragments were dislocated to the antero-medial position and overlapped the ramus.(Fig. 8) Postoperative radiographs showed good anatomical reduction of both condylar fragments in the glenoid fossa.(Fig. 9. A, 9. B) On postoperative 5-month radiographs, there were signs of displacement and rotation of the right condylar fragment with plate fractures and screw loosening.(Fig. 9. C) The postoperative 6-month radiograph showed bone remodeling at the displaced fracture site with increased radiodensity. Finally, complete remodeling of both condylar fragments was observed on the postoperative 8-month radiograph.(Fig. 9. D) There were no signs or symptoms of mandibular condylar dysfunction during the remodeling period.
III. Discussion
There are many treatment options for management of mandibular condylar fractures, including open reduction through an intraoral or extraoral approach and closed reduction. The prognosis for each treatment is very controversial1.
Hidding et al.2 compared ORIF (20 cases) and CRMMF (14 cases) and found that deviation on mouth opening occurred in 64% of cases in the CRMMF group compared with 10% in ORIF group. In addition, anatomic reconstruction of the condyle was seen in 93% of the ORIF group but only 7% of the CRMMF group.
According to Zide and Kent3 and Zide4, there are absolute and relative indications for open reduction, such as bilateral condylar fracture, extracapsular dislocation, and displacement of the condyle. This seems to be supported by the work of Silvennoinen et al.5, who have demonstrated an increased frequency in temporomandibular joint (TMJ) dysfunction and occlusal disorders when unilateral condyle fracture demonstrating dislocation or significant loss of ramus height as treated nonoperatively with inter-maxillary fixation only.
Open reduction and fixation are necessary to maintain the anatomic reduction of the condyle and the height of the ramus. However, in cases of high condyle fracture or displacement or dislocation of the condyle to the antero-medial side, it can be difficult to secure a field of vision during open reduction. Although a preauricular or endaural approach is used to obtain field of vision, there is a possibility of nerve damage due to the adjacent facial nerve. Also, surgical difficulty remains an issue due to the narrow field of view and work space6.
Extracorporeal reduction is one possible method to solve this problem. Through removal of the ramal part by vertical ramal osteotomy, this procedure can obtain a view of the condylar fracture site and easy handling of the instrument. It is also accurate and relatively easy because reduction and internal fixation are performed out of body7.
However, extracorporeal reduction implies that fractured condylar fragments are separated from the TMJ capsule. In other words, the soft tissues including the lateral pterygoid muscle are completely detached, increasing the risk of condylar resorption, such as with a free graft89.
Davis et al.8 reported that advanced condylar resorption occurred in 3 out of 10 patients who underwent free-grafting of the fractured condyle. Iizuka et al.10 reported less encouraging results in 10 free-grafted patients with miniplate fixation for high condylar fractures, reporting ‘significant resorption’ in 85% of cases.
In 1995, Pereira et al.9 reported the clinical and radiological results of surgical treatment of 17 patients with 21 dislocated fractures of the condylar process of the mandible. In this series, in all cases in which the lateral pterygoid muscle remained attached to the fractured segment, x-ray and tomography images confirmed a normal shape and contour of the condylar process. On the other hand, in those cases in which the fractured segment was maintained as a free graft, the majority (12 of 13 patients) showed signs of resorption of the condylar process with resulting shortening of the vertical dimension of the mandible and signs of remodeling, especially of the mandibular fossa, which became flat or even convex.
Therefore, prevention of condyle resorption can be expected if intracorporeal reduction of condylar fracture was performed using both pedicled condylar and separated ramal fragments after vertical ramal osteotomy. Reduction of a condylar fragment to a separated ramal fragment in the intracorporeal state without detaching the lateral pterygoid muscle from the condylar fragment can be more difficult than in the extracorporeal state. However, displacing the ramal part medially and pulling down the condylar fragment can provide a field of view and work space even though it is not convenient.
In our study, Case 1 had undergone SPECT at postoperative 1 week. Blood supply to the condylar and osteotomized ramal fragments was suspected due to hot spots on the left fragments in SPECT.(Fig. 5) Tc-99m accumulates in areas of increased bone formation and increased angiogenesis, allowing visualization of inflammation. Because fracture healing involves inflammation, reparative, and remodeling phases, the hot spots are believed to be evidence of angiogenesis in the inflammation phase of fracture healing.
However, there are very few studies using SPECT for condylar fractures. Therefore, comparative studies with extracorporeal reduction or long-term follow-up studies are necessary.
In Cases 2 and 3, diagnosed as bilateral condylar fractures, there were signs of condylar displacement accompanied by plate fractures and screw loosening on 1- or 5-month radiographs. However, postoperative 8-month or 2-year radiographs showed bone remodeling at the displaced fracture site with increased radiodensity. This suggests that the fragments had vitality due to maintained blood supply at the fracture site. As a result, complete remodeling of condylar fragments with restored anatomic appearance was observed on all final follow-up radiographs.(Fig. 7. D, 9. D) There were no symptoms of condylar dysfunction during the healing and remodeling periods.
Condylar resorption is avascular necrosis with consequent shortening and loss along the vertical dimension of the mandible. In this paper, the definition of condylar resorption was resorption of more than one-third of the condyle length compared with the condyle dimension immediately after treatment or on the opposite side of the condyle11.
Remodeling is a state of healing after fracture. The shapes of condylar fragments can be changed by a mechanical element, but the vertical dimension of the mandible is maintained.
Complete detachment of the soft tissue from the ramal and condylar fragments increases the risk of avascular necrosis as with a free graft, which can lead to condylar resorption. To prevent avascular necrosis, intracorporeal reduction of a condylar fracture using both pedicled condylar and separated ramal fragments after vertical ramal osteotomy was performed. As a result, despite displacement of fragments in the bilateral condylar fractures, condylar resorption was not observed on postoperative 8-month or 2-year radiograph, and anatomical appearance was maintained.
When calcification is increased, a hard callus can be observed in the panorama, indicating that hard callus forms 20 to 60 days after surgery. The remodeling phase, the last stage of healing, is a long, slow process that lasts from months to years. Davis et al.8 reported that, of 10 patients who had undergone 11 free graft procedures, three required secondary costochondral reconstruction due to advanced resorption of the free-grafted condylar segment, occurring from 3 to 9 months following the initial trauma surgery.
Therefore, follow-up is needed at 3 months postoperatively because radiological changes can be observed and also at 1 year postoperatively to assess the remodeling phase.
Case 1 might require a longer follow-up period to evaluate condylar resorption. No condylar resorption was observed on postoperative 8-month or 2-year radiograph, and anatomical appearance was maintained in Cases 2 and 3, respectively.
It is obvious that restoring the vertical height through anatomical reduction and preventing avascular necrosis will reduce the risk of complications such as deviation on mouth opening and TMJ dysfunction.
Meanwhile, there were signs of condylar displacement accompanied by plate fractures and screw loosening on 1- or 5-month radiograph in Cases 2 and 3, respectively.
There are two major causes of plate fracture or screw loosening. The first cause is the force generated by the masticatory muscles; the second is the force produced by biting. In particular, the condylar fragments were loaded with direct force from the lateral pterygoid muscle, and the mandibular body and angle are also affected by the medial pterygoid muscle and the masseter muscle. Therefore, various forces such as bending and torsion are loaded onto the fracture line and the plate12.
Double plate fixation can be considered as a solution to this problem. In Case 2, a single plate was used. Some authors reported plate fracture or screw loosening after application of a single miniplate for condylar fracture and mentioned that single miniplate fixation might be insufficient for reduction and fixation of condylar fracture1012.
Tominaga et al.12 reported that double adaptation plate fixation resulted in superior biomechanical stability in both fracture conditions in a laboratory setting.
However, in Case 3, plate fracture and screw loosening occurred after double plate fixation. In Case 3, we started mouth movement exercise two week after surgery to reduce TMJ complications, which is thought to be the stage of soft callus. Early mouth opening exercise can reduce TMJ complications, but can also reduce the stability of the internal fixation. Therefore, if the intermaxillary fixation period is increased to more than 2 weeks, the stage of soft callus can be prolonged, and the mechanical support can be increased, which could be a solution to the complication observed in Case 3.
In conclusion, all cases exhibited good healing aspects with no signs or symptoms of mandibular condylar dysfunction during the postoperative remodeling period after intracorporeal reduction of condylar fracture.






 XML Download
XML Download