

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Synovial chondromatosis is a rare, intra-articular, benign bone lesion that leads to the formation of a large number of cartilaginous or osteochondromatous nodes within the synovial fluid and intra-articular loose bodies1. It most frequently develops in the knee, elbow, wrist, and shoulder2. When occurring at the temporomandibular joint (TMJ), synovial chondromatosis usually develops in the superior joint space, and infiltration of the skull is very rare3.
While the causes of synovial chondromatosis are not clearly known, embryological causes, degenerative joint lesions, continued stimulus of the affected articular disc, injury, and inflammation are considered possible causes. Lesions caused by embryological factors present as rather aggressive, while those caused by an injury or inflammation are chronic and less aggressive34.
Clinical symptoms displayed by patients with synovial chondromatosis resemble common symptoms of TMJ disorder such as pain and swelling around the TMJ, mouth opening limitation, and joint sounds; abnormal occlusion with crossbite and facial asymmetry are present in more severe cases5.
We report rare cases of synovial chondromatosis that invaded the joints and skull in the upper direction and present a literature review.
II. Cases Report
1. Case 1
A 26-year-old female patient visited the Department of Neurology at our institution with a chief complaint of headache and was referred to our department after lesions in the right cranial base and TMJ were discovered on magnetic resonance imaging (MRI). The patient did not have an unusual medical history, and no unusual symptoms were observed regarding the TMJ other than sharp pain in the left temporal region opposite the lesion. No unusual observation was made on the panoramic radiographs or computed tomography (CT) scans of the TMJ obtained in the first medical examination. On the MRI scans, the lesions were surrounded by a film that measured 11×11×7 mm and was positioned above the right temporal bone joint and TMJ. Within the lesion, a mix of high intensity and low intensity signals were observed on both T1 and T2 images.(Fig. 1) Erosion and communication with the right TMJ were observed in the base of the right temporal bone.(Fig. 2. A, 2. B)
After inducing anesthesia through nasotracheal intubation, open surgery was performed on the right TMJ using the preauricular approach. The superior joint space was exposed via open reduction while ensuring that the facial nerves were intact. No leakage of synovial fluid occurred upon exposure of the superior joint space, and no degenerative changes of the articular disc were observed. Loose bodies were found in the base of the glenoid cavity and were removed via curettage. A hole 2 mm in diameter was observed in the middle of the glenoid cavity. A lesion that extended to the skull through the pore contained loose bodies.(Fig. 3) The dura mater was exposed following the removal of the lesion, but no cerebrospinal fluid (CSF) leak occurred. The exposure site was closed with Tachocomb (Nycomed International Management, Zurich, Switzerland), a type of collagen matrix barrier.
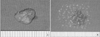
Biopsy results showed clusters of synovial fibroblasts (Fig. 4. A) and typical cartilage cells (Fig. 4. B). The patient was finally diagnosed with synovial chondromatosis.
No important symptoms other than decreased sensations in the ipsilateral side and tinnitus were observed, and the patient no longer complained of a headache. Two weeks after the open surgery of the TMJ, a maximum jaw range of motion (ROM) of 25 mm was noted, which returned to the normal value of 50 mm at 6 months after the surgery. Symptoms that caused discomfort, including tinnitus and decreased sensations, were also relieved.
CT scans obtained before and after the surgery showed complete removal of the lesion in the right cranial base.(Fig. 2) CT scans obtained 7 days after the surgery showed that approximately 2 mm of the area left by lesion removal was filled with air, which confirmed that neither perforation of the meninges nor brain herniation occurred. CT scans obtained at 3 months and at 2.5 years after the surgery showed reossification and satisfactory recovery of the defects caused by the lesion.(Fig. 2. C–F)
2. Case 2
A 31-year-old female patient visited the clinic with a chief complaint of pain in the TMJ. The maximum jaw ROM was 45 mm, and the patient complained of pain in the left TMJ when opening her mouth. T2 scans in MRI showed a lesion with a high-intensity signal and low-intensity signals possibly originating from loose bodies above the glenoid fossa and articular eminence.(Fig. 5) CT scans showed condylar erosion in the left TMJ and no calcification.(Fig. 6. A)
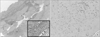
The patient was diagnosed with synovial chondromatosis of the left TMJ based on these examination results, and surgery was performed accordingly. A preauricular approach extending to the left temporal region in to the glenoid cavity was used after inducing general anesthesia. A flat, soft, beige mass from the superior joint space was weakly attached to the middle of the glenoid cavity and was easily removed. A bone defect formed in the upper direction from the center of the glenoid cavity measured 5 mm in diameter and 1.5 mm in depth. Another defect located at the articular tubercle measured 10 mm in diameter and 7 mm in depth and was filled with a grayish-brown mass of soft tissue.(Fig. 7) No hole was observed in the glenoid cavity. The articular disc was relatively easily restored. It was confirmed that there was no functional deformity of the articular disc after securing the space via eminoplasty. After sufficiently rinsing the inside of the glenoid cavity, a 0.02-inch silastic sheet was placed in the glenoid cavity and sutured. Biopsy results showed synovial fibroblasts and cartilage cells.(Fig. 8) The patient was finally diagnosed with synovial chondromatosis. No symptoms of relapse were observed during the follow-up for 6 months after the surgery.(Fig. 6. B)
III. Discussion
Synovial chondromatosis is a benign lesion that develops in large joints of the limbs such as the knee, hipbone, shoulder, and elbow, and rarely in jaw joints. While the causes of synovial chondromatosis have not been clearly identified, the occurrence can be due to metaplasia of the synovial mesenchymal cells, injury or joint disease6.
Synovial chondromatosis developing in a jaw joint can cause a variety of clinical symptoms, such as swelling and pain in the affected region, crepitation when opening the mouth, and mouth opening limitation. However, in some cases, no unusual symptoms are observed around the jaw joints, as occurred in the first patient discussed in this study. In addition, due to chronic, gradual swelling, synovial chondromatosis can be misdiagnosed as dysplasia of the mandibular condyle, osteochondromatosis, tumor in the preauricular region, or lesions in the parotid gland789.
Synovial chondromatosis exhibits CT characteristics similar to osteoarthritis in terms of enlargement of intra-articular spaces, soft tissue swelling, irregularity of joint surface, hyperostosis of the glenoid cavity, and osteosclerosis. A unique characteristic of synovial chondromatosis is that loose bodies, which are an end product of cartilaginous metaplasia, can be observed. In some cases, these loose bodies can be calcified. Exudation and accumulation of synovial fluid can be observed on MRI and can help determine whether or not a lesion is of synovial origin. Therefore, it is recommended to perform both CT and MRI before surgery1011121314.
Synovial chondromatosis can be histologically differentiated into 3 stages. In the early activation stage, it is characterized as a lesion within the synovia that develops without the formation of any loose bodies. In the middle stage, accumulation of synovial fluid within the glenoid cavity and loose bodies can be observed. In the final stage, loose bodies can still be observed, but the synovial fluid exhibits normal characteristics15.
For differentiation of synovial chondromatosis from chondrosarcoma, a histological examination is necessary. Once the absence of necrosis, mixed cartilage, activation of nuclear differentiation, and fusiform cells is confirmed, the lesion can be confirmed benign16.
Cases of progression of synovial chondromatosis to a malignant lesion in knee joints have been reported, but are very rare. As the recurrence of a lesion in these areas is also reported at low rates17, it is considered a benign lesion with a good prognosis.
Of the 47 patients who were diagnosed with synovial chondromatosis of the TMJ and had the lesion removed at our institution between 1990 and 2016, 43 had lesions confined to the superior joint space, and 2 had lesions confined to the inferior joint space; only 2 cases (4.25%) showed extension into the skull and erosion of the base of the temporal bone.
Synovial chondromatosis usually develops in the superior joint space, rarely extends to the skull, and gives rise to symptoms associated with TMJ disorder18. When it occurs in the inferior joint space, it can extend to the mandibular condyle and surrounding structures. In this case, additional surgical procedures such as a condylectomy might be required19.
When synovial chondromatosis extends to the skull, the dura mater can become exposed, and a CSF leak can occur; collaborative treatment with a department of neurosurgery must be considered5. Dura mater repair might be necessary in some cases.
In the first patient discussed in the present case report, although the lesion invaded the skull, no unusual symptoms were noted other than a headache on the contralateral side in the first medical examination. The second patient complained of pain around the TMJ area ipsilateral to the lesion when opening the mouth, a symptom that did not significantly differ from typical symptoms of TMJ disorder. By the end of the follow-up that lasted 2.5 years after the lesions were removed through open surgery on the TMJ, the aforementioned symptoms were relieved for both patients, and no recurrence occurred.






 XML Download
XML Download