

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Oral cancer is the sixth most common malignancy and is a major cause of cancer morbidity and mortality worldwide1. More than 90% of tumors that originate in the head and neck area are squamous cell carcinoma (SCC), a tumor of epithelial origin. Oral squamous cell carcinoma (OSCC) can be preceded by clinically evident premalignant lesions. Among the premalignant lesions, leukoplakia is the most commonly encountered lesion and can show varying degrees of epithelial dysplasia ranging from mild to severe. The likelihood of developing an invasive carcinoma increases with the severity of dysplasia. The frequency of carcinomatous changes in oral leukoplakia varies from 6.6% to 36%2.
Immunohistochemical (IHC) studies have investigated OSCC to better understand the biology, diagnosis, prognosis, and treatment3. Rapid progress has been made in the last several years to elucidate the underlying cell cycle regulation and other molecular mechanisms in mammalian cells. Cyclin D1, a 45 kDa protein, is part of the molecular system that regulates the cell cycle G1 to S transition4. Dysregulation of the cell cycle machinery is a fundamental hallmark of cancer, and this is emerging as a central theme in oral carcinogenesis. Therefore, the genes involved in cell cycle control represent targets for oncogenic abnormalities, and cyclin D1 could prove to be a worthwhile target for treatment approaches3.
p63 protein has been regarded as a novel basal cell IHC marker. A dual role of p63 protein has been reported56. p63 protein is expressed in the proliferative layer of cells near the basement membrane of the normal oral mucosa, where it likely prevents basal cells from differentiating and thereby helps to maintain their basal cell status. However, upon dysplastic change (i.e., transition from normal oral mucosa to epithelial dysplasia), dysplastic keratinocytes above the basal layer can shift to a status similar to the embryogenesis condition and are still able to express p63 protein, which produces an antidifferentiation effect as well as a proliferative capacity of dysplastic cells in the oral dysplastic mucosa. p63 can contribute to the development of epithelial dysplasia by altering stem cell function in the basal layer, resulting in an increased number of proliferating cells, and this can contribute to the altered distribution in basal and suprabasal layers within oral epithelial dysplasia47.
This study of cyclin D1 as well as p63 expression indicated that these gene products can be useful for a more precise diagnosis of leukoplakia and OSCC.
II. Materials and Methods
This was a laboratory-based study that involved using 10% neutral buffered fixed formalin and representative paraffin-embedded histopathologically-diagnosed tissue cases of OSCC and leukoplakia, which were retrieved from the Department of Oral and Maxillofacial Pathology, K.M.Shah Dental College and Hospital (Vadodara, India). The samples were retrieved after the study was approved by the ethical committee of the institution, K.M.Shah Dental College and Hospital.
A total of 60 cases, comprised of leukoplakia and OSCC, were evaluated for p63 and cyclin D1 expression. The study included 30 cases of OSCC and 30 leukoplakia cases. OSCC was grouped into 3 categories based on Broder's histopathological grading: well-differentiated (WDSCC), moderately-differentiated (MDSCC), and poorly-differentiated (PDSCC) carcinoma.
Leukoplakia tissues were subdivided according to the World Health Organization classification from 2005, using the architecture and cytology criteria of mild dysplasia, moderate dysplasia, and severe dysplasia.
1. Immunohistochemistry
Two to three serial sections, 4 µm thick, were placed on silanized slides for p63 and cyclin D1 IHC staining. The protocols for both markers were performed according to the manufacturer's recommendations. The sections were deparaffinized and rehydrated through changes of xylene and descending grades of alcohol. Antigen retrieval was carried out in citrate buffer with a pressure cooker for 5 minutes. The pressure cooker was allowed to cool to room temperature with the slides remaining in the buffer for 15 to 20 minutes.
The sections were incubated with peroxidase blocking reagent for 15 minutes, followed by incubation with ready to use monoclonal p63 and cyclin D1 antibody (Dako EnVision FLEX system; Dako, Glostrup, Denmark) for 1 hour at room temperature.
After additional incubation with secondary antibody for 45 minutes, visualization was performed using freshly prepared substrate chromogen solution for 10 minutes. The slides were then counterstained with Harri's hematoxylin for 2 minutes. The presence of brown colored end product at the site of target antigen was indicative of positive immunoreactivity. The absence of staining in the negative control tissue demonstrated specificity.
The positive results were further assessed for intensity of staining, which was graded for statistical analyses. In cases with staining heterogeneity, the expression was grouped according to the predominant staining intensity as (+) mild staining, (++) moderate staining, and (+++) intense staining based on a study by Castle et al.8. All observations were performed by two more observers in order to eliminate interobserver bias.
2. Statistical analyses
A chi-square test was used for comparison and correlation between leukoplakia and OSCC and between grades of dysplasia and OSCC. Statistical significance was defined as P<0.05. The data collected were analysed statistically using SPSS Statistics ver. 17 (SPSS Inc., Chicago, IL, USA).
III. Results
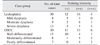
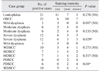
Cyclin D1 positivity was seen in 21 cases (70.0%) of leukoplakia in Fig. 1. A and 23 cases (76.7%) of OSCC in Fig. 1. B. Mild dysplasia (37.5%), moderate dysplasia (66.7%), and severe dysplasia (92.3%) were identified, and OSCC grades included WDSCC (66.7%), MDSCC (87.5%), and PDSCC (85.7%). These dysplasia and OSCC grades showed (Table 1) p63 positivity in all cases of leukoplakia in Fig. 1. C and OSCC in Fig. 1. D.(Table 2) Statistical significance at P<0.05 was observed for cyclin D1 and p63 expression between 2 categories of dysplasia and OSCC.(Tables 3, 4) Higher levels and increased expression of cyclin D1 and p63 were found in different grades of dysplasia in leukoplakia cases, as shown in Table 5. Similarly, the expression of both cyclin D1 and p63 was pronounced in well-differentiated SCC. However, the intensity of both cyclin D1 and p63 expression was also notable in poorly-differentiated SCC.(Table 6) Comparison of both cyclin D1 and p63 expression in different grades of dysplasia of leukoplakia cases showed no statistically significant differences. Cyclin D1 expression was highly significant compared to severe and mild grades of dysplasia.(Table 7) Both cyclin D1 and p63 expression was statistically significant compared with poor grades of SCC, as shown in Table 8.
IV. Discussion
Many studies have assessed SCCs, with a primary objective to understand the biology and determine the severity and prognosis of oral cancers with diverse behavior8. The cell cycle impacts the complexity of growth, renewal, and repair in all organisms9 and can be visualized as a relay race consisting of G1, S, G2, M, and G0 phases. Each of these laps is regulated by a distinct set of “cyclins” that activate their CDK partners and propel the cell forward in its proliferative pool. Negative control over the cell cycle is exerted by CDK inhibitors10.
Cancer cell escape from the cell cycle machinery reflects a fundamental hallmark of cancer progression and is emerging as a central theme in oral carcinogenesis3. Indeed, the strongest connection between cyclins and oncogenesis was shown in studies on cyclin D111. The underlying mechanisms for cyclin D1 overexpression include gene amplification, chromosomal translocation, and other post translational mechanisms312.
This study utilized the cyclin D1 monoclonal antibody for OSCC to elucidate the role of this key cell cycle regulator in this neoplasia. In our study, 21 cases (70.0%) of leukoplakia showed cyclin D1 positive expression, which is slightly lower than the findings reported by Castle et al.8, which found 84.62% positive expression. Eleven cases (52.38%) showed mild, 7 cases (33.33%) showed moderate, and 3 cases (14.29%) showed intense cyclin D1 expression. These findings were similar to Castle et al.8 who found that 45.45% of patients showed mild, 40.90% showed moderate, and 13.63% showed intense cyclin D1 expression. All positive mild dysplasia cases showed mild expression, while 50% of severe dysplasia cases showed moderate to intense expression, which shows that the cyclin D1 expression increased in parallel with the severity of dysplasia.
Twenty-three cases (76.7%) of OSCC showed positive cyclin D1 expression, which is slightly higher than studies reported by Angadi and Krishnapillai13, Lam et al.14, and Goto et al.15, which found 70.73%, 63%, and 65.9% positive cyclin D1 expression, respectively. In this study, 60% of WDSCC cases showed mild to moderate expression that was similar to results reported by Angadi and Krishnapillai13 (46.9%) and Goto et al.15 (67.74%). All PDSCC cases showed moderate to intense cyclin D1 expression, which is also in concordance with Angadi and Krishnapillai13 (88.90%). In addition, Goto et al.15 (100%) indicated that cyclin D1 expression increases and is correlated with poor histological grade. The difference in expression was statistically significant (P<0.05). Moreover, cyclin D1 overexpression has been reported in various diverse histogenesis tumors, such as breast carcinomas16, hepatocellular carcinomas17, endometrial carcinoma18, colon carcinomas16, esophageal carcinoma1920, and lung carcinoma12.
p63 is a p53 homologue that plays a distinctive role in the physiology of the epithelium. TAp63, like p53, exhibits tumor-suppressive properties, while up-regulation of ΔNp63 isoforms is common and a distinctive feature of tumorigenesis21. The role of p63 in oral dysplasia and tumors has been the focus of numerous studies, although the results remain conflicting. It is widely accepted that normal and non-dysplastic mucosa show nuclear expression of p63 in the basal and parabasal keratinocytes of the epithelium, with the major functioning isoform being ΔNp63. As dysplasia increased in severity, the percentage of p63 positive cells increases and extends into the upper epithelial layers. In addition, overexpression of p63, especially ΔNp63, is frequently seen in HNSCC tumors and HNSCC-derived cell lines22232425. Additionally, oral leukoplakia with increased ΔNp63 expression and inflammatory cell infiltration exhibits a higher rate of cancer development and worse prognosis26.
In our study, all cases of leukoplakia showed p63 expression, which is similar to studies by Takeda et al.27, Chen et al.24, Vered et al.28, Bortoluzzi et al.23, and Choi et al.29. In the present study, 62% cases of mild dysplasia showed mild expression, while 66.54% cases of severe dysplasia showed moderate to intense expression. Thus, p63 expression increased parallel to the severity of dysplasia, similar to findings of Takeda et al.27. In addition, all cases of OSCC showed positive p63 expression. This finding is correlated with reports from other studies of Sakiz et al.30, Moergel et al.31, Chen et al.24, Bortoluzzi et al.23, Chen et al.32, Faridoni-Laurens et al.33, and Choi et al.29, who reported 100% positive p63 expression.
Out of 30 OSCC cases, 11 cases (36.7%) showed mild, 13 cases (43.3%) showed moderate, and 6 cases (20.0%) showed intense p63 expression. This is similar the results of a study by de Oliveira et al.25, who found 31.1% mild, 50% moderate, and 18.9% intense p63 expression. The results indicated that 93.33% cases of WDSCC showed mild to moderate, 62.5% cases of MDSCC showed moderate, and 100% cases of PDSCC showed intense p63 expression, indicating that p63 expression increased with poor histological grade. This result was statistically significant (P<0.05).
A literature search indicated that very few studies have reported isolated examination of either leukoplakia or OSCC. This study involved both cyclin D1 and p63 expression in leukoplakia as well as all grades of OSCC. The expression of both cyclin D1 and p63 increased as the stage of dysplasia in leukoplakia cases increased from mild to severe.(Table 5) The total cyclin D1 and p63 expression was more general with well-differentiated SCC. In contrast, the intensity of OSCC in poorly-differentiated cases was greater than that in well- and moderately-differentiated SCC.(Table 6) This indicates that the cancer prognosis is evident from increased expression as dysplasia increases, which is in accordance with Todd et al.3.
Overexpression of p63 has been reported in various tumors, including adenocarcinoma and SCC3435, adenoid carcinoma, polymorphous low-grade adenocarcinoma and basal cell and canalicular adenomas36, esophageal carcinoma6, and prostate cancer7. p63 expression was mainly noted in the peripheral cells of tumor nests in the well-differentiated tumor area, similar to a report by Chen et al.32.
The overall expression of cyclin D1 and p63 correlates with poor histological grades of OSCC and leukoplakia. The increased cyclin D1 and p63 expression parallel with the severity of lesions likely reflects the intense proliferative activity and invasiveness of these lesions. In general, cyclin D1 and p63 expression increased with increased grade of dysplasia in leukoplakia and OSCC.
V. Conclusion
In this study, we conclude that cyclin D1 and p63 are involved in carcinogenesis, which is associated with changes from early dysplasia to poorly-differentiated carcinoma, and these changes are noted with higher expression patterns in leukoplakia and OSCC. We found a significant association between increased cyclin D1 expression in mild and severe dysplasia in leukoplakia cases, but not with other groups (mild vs moderate and moderate vs severe).(Table 7) Hence, the results indicate that the severity of dysplasia increases with increased expression of cyclin D1 and can indicate a high risk for malignant transformation. Cyclin D1 and p63 expression was significantly higher than that in well-differentiated SCC and poorly-differentiated SCC, respectively.(Table 8) IHC demonstration of these gene products can be a useful tool for a more precise prognosis of leukoplakia and OSCC. Similar studies with a larger sample size in different areas of the oral cavity and that assess all stages of SCC will provide additional insight into oral carcinogenesis and the roles of cyclin D1 and p63.







 XML Download
XML Download