

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
The number of cases of carcinoma of the lips and oral cavity worldwide was about 300,000 in 2012, or 2.1% of all carcinomas that year12. Among them, squamous cell carcinoma was most common among males aged over 60 years who drank and smoked345. In recent years, however, the incidence has been increasing in women 40 years and below who do not have these same cancer risk factors678.
Oral squamous cell carcinoma (OSCC) is treated with surgery, radiotherapy, and chemotherapy, often in combination. For patients in early TNM stages I and II, the effect of a single surgical treatment or radiotherapy was not statistically significant9. However, for patients in a more advanced TNM stage (III or IV), the combination of surgical and radiotherapy showed the best therapeutic effect10.
The TNM staging, especially for lymph node metastasis, is the scoring system most widely used among prognostic factors for patient survival1112. Several biomarkers have been studied as serologic markers, but their specificity is low and clinical applications are difficult13. It is essential that clinicians discover effective and clinically efficient biomarkers as prognostic factors for OSCC.
In studies conducted over the last few decades, platelet activation has been considered an important biological process for cancer occurrence and metastasis141516. Platelet (PLT) and mean platelet volume (MPV) are the most common measures of platelet activation17, and high MPV levels indicate abnormal platelet production and activation18. Recent studies have shown that MPV levels are relatively high in tumor patients, and that prognosis was poor in patients with gastric tumors showing relatively high MPV levels192021. There have been no studies conducted on the application of both PLT and MPV level in predicting postoperative survival in patients with OSCC.
This study aimed to establish a scoring system for OSCC patients using PLT and MPV levels measured postoperatively and to evaluate their significance as prognostic factors.
II. Materials and Methods
1. Patients
We studied 40 patients admitted to the Department of Oral and Maxillofacial Surgery of Dankook University Hospital (Cheonan, Korea) who were diagnosed with primary OSCC histopathologically between May 2006 and May 2012. Patient cases were excluded for any of the following reasons: (1) experienced severe complications or died within 30 days after surgery, (2) experienced preoperative systemic inflammatory response syndrome, (3) had infections or autoimmune diseases, or (4) had recently undergone radiotherapy or chemotherapy. A total of 40 patient cases were included in the study.
Clinical pathological information obtained from the medical records of each patient included age, sex, height, weight, tumor location, degree of differentiation, tumor diameter, lymph node metastasis, and TNM stage. TNM stage was diagnosed according to the American Joint Committee on Cancer (AJCC) 7th edition and other test values including white blood cell (WBC), MPV, PLT, C-reactive protein (CRP), and albumin obtained through a test conducted within 7 days before surgery. We conducted this study in compliance with the principles of the Declaration of Helsinki. Due to the retrospective nature of this study, it was granted written exemption by the Dankook University Dental Hospital's Institutional Review Board. The informed consent was waived.
2. Count of platelet and mean platelet volume (COP-MPV) score system
The cut-off values of PLT and MPV were determined by receiver operating characteristic (ROC) curves. Groups were divided as described below. The cut-off value for PLT was 263.5×109 L−1 and for MPV was 10.15 fL. Patients with both PLT and MPV values below cut-off were defined as score 0 (group A). Patients with at least one of the two higher than cut-off were defined as score 1 (group B).
Neutrophil-lymphocyte ratio (NLR) and platelet-lymphocyte ratio (PLR) were calculated by dividing absolute neutrophil and PLT by absolute lymphocyte count.
3. Statistical analysis
Overall survival was defined as the period of time to the patient's death or the period of time to the date when last follow-up was performed. In order to compare significance between groups, categorical variables were expressed as a percentage using the χ2 test and continuous variables that were normally distributed were expressed through regularity tests. For continuous variables that did not follow a standard distribution, the mean of the two groups was compared using the Mann-Whitney U test and then expressed as mean±standard deviation. Cut-off values for all continuous variables were determined using ROC curves. Variables with P-values less than 0.05 were considered significant prognostic factors through univariate analysis. The effect of these variables on survival rate was analyzed using a multivariate Cox proportional hazards model. Kaplan-Meier curves and log-rank tests were used to determine the difference in survival rate between groups. IBM SPSS Statistics 21.0 software (IBM Co., Armonk, NY, USA) was used to conduct statistical analyses. P-values less than 0.05 were considered statistically significant.
III. Results
1. Patient characteristics
A total of 40 patients (28 males and 12 females) were included in this study. The mean age at the time of diagnosis was 64.08±11.59 years (median age, 66 years; range, 35–88 years). The mean follow-up period was 32.58±22.49 months (range, 3.7–82.0 months) and 11 patients died during the observation period. For TNM stage, 10 patients (25.0%) were stage I, 7 patients (17.5%) were stage II, 6 patients (15.0%) were stage III, and 17 patients (42.5%) were stage IV. Primary tumors were located on the lips in 2 patients (5.0%), on the buccal mucosa in 3 patients (7.5%), on the floor of the mouth in 3 patients (7.5%), on the gum in 12 patients (30.0%), in the maxillary sinus in 2 patients (5.0%), and on the retromolar pad in 4 patients (10.0%). Mean PLT and MPV were 243.93±61.382 ×109 L−1 (103–389 ×109 L−1) and 10.05±0.67 fL (8.8–11.4 fL), respectively. Other parameter values and ranges were as follows: WBC, 6.44±1.79 ×103/µL (3.52–10.83 ×103/µL); albumin, 4.14±0.45 g/dL (2.6–4.8 g/dL); CRP, 0.52±0.79 mg/dL (0.02–4.61 mg/dL); PLR, 127±39.51 (37.73–252.46); NLR, 1.92±0.76 (0.53–3.89); and maximum tumor size, 2.75±1.36 cm (0.8–5.9 cm).
2. Clinicopathological characteristics between COP-MPV groups
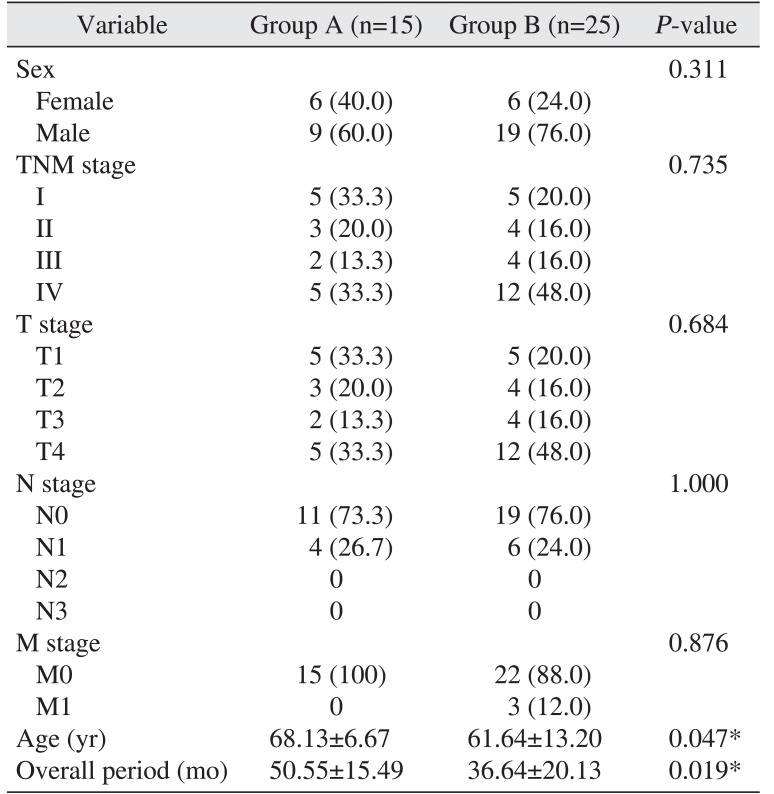
The mean age at the time of clinicopathological characteristic measurement for COP-MPV group A was older (68.13±6.67 years) than group B (61.64±13.20 years) (P=0.047). The COP-MPV group A was in the study longer on average (50.55±15.49 months) than the COP-MPV group B (36.64±20.13 months) (P=0.019). There was no statistically significant relationship with age (P=0.311), N-metastasis (P=1.000), or TNM stage (P=0.735).(Table 1)
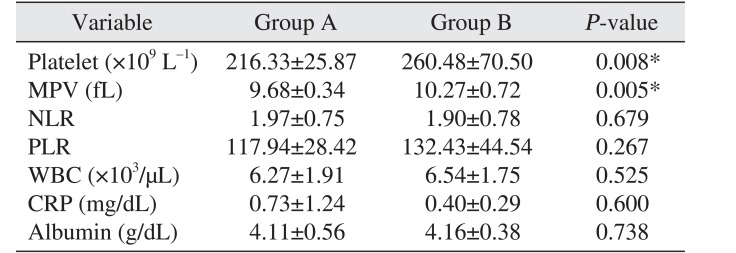
The PLT of the COP-MPV group A was 216.33±25.87 and that of the COP-MPV group B was higher 260.48±70.50 (P=0.008). The MPV level of the COP-MPV group A (9.68±0.34) was lower than that of COP-MPV group B (10.27±0.72) (P=0.005). There was no statistically significant relationship with NLR (P=0.679), PLR (P=0.267), WBC (P=0.525), CRP (P=0.600), or albumin (P=0.738).(Table 2)
3. Univariate analyses
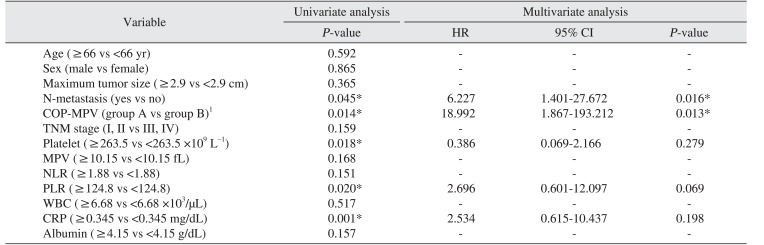
Clinical and laboratory variables were divided into groups based on their respective cut-off values and the relationship between overall survival and each respective variable was analyzed. Univariate analyses showed N-metastasis (P=0.045), COP-MPV (A vs B) (P=0.014), PLT (≥263.5 vs <263.5 ×109 L−1) (P=0.018), PLR (≥124.8 vs <124.8) (P=0.020), and CRP (≥0.345 vs <0.345 mg/dL) (P=0.001) were statistically significant prognostic factors.(Table 3)
4. Multivariate analyses
A multivariate Cox proportional hazards model was used with univariate analyses to determine the significance of variables with a P-value less than 0.05 as independent prognostic factors for OSCC patients. Results were as follows: N-metastasis (HR 6.227, 95% confidence interval [CI] 1.401–27.672, P=0.016); COP-MPV (A vs B) (HR 18.992, 95% CI 1.867–193.212, P=0.013), indicating both N-metastasis and COP-MPV were significant independent prognostic factors for OSCC patient survival.(Table 3)
5. Kaplan-Meier analyses
Kaplan-Meier analyses were used to determine the difference in overall survival between COP-MPV groups. The prognosis of COP-MPV group B was worse than that of COP-MPV group A (P=0.014). The prognosis of the group with lymph node metastasis was worse than that of the non-metastasis group (P=0.018).(Fig. 1, 2)
IV. Discussion
Recent studies have provided evidence that platelet activation is clinically significant in some malignant tumors. In particular, in a series of processes in which cancer cells spread to other organs through blood circulation, platelets are important for cancer cells to aggregate and be discharged from blood vessels2223. Some studies have reported that, in cancer patients, platelet activation indexes (soluble P-selectin, soluble CD40 ligand, and platelet factor 4) are relatively higher than in normal patients242526. Some studies have reported that MPV is also closely related to various thromboembolic disorders including ischemic cardiovascular disease2728, and some studies have reported that MPV is related to malignant tumors1929. However, whether the prognosis of patients with relatively high MPV is worse than those with low MPV remains a subject of debate. Osada et al.30 reported that MPV level rose in malicious tumors such as gastric cancer. In contrast, Mutlu et al.31 did not find any elevation in MPV level in various cancer patients and, compared with time of first cancer diagnosis, MPV level was significantly reduced at the time of thrombotic events. However, larger platelets secrete more chemical mediators upon stimulation than smaller ones, and the increase in number of larger platelets suggests that stimulation exists from diseases such as cardiovascular disease or malignant tumors272830. PLT and MPV are important indexes for assessing platelet activation state17. It is essential to predict the prognosis of OSCC patients using a scoring system that includes comprehensive consideration of PLT and MPV.
The mean age of group A was higher (68.13 years) than group B (61.64 years), indicating that age was lower in group B with poor prognosis (P=0.047).(Table 1) Goldstein and Irish32 and Sarkaria and Harari33 found in their study that squamous cell carcinoma in the head and neck showed a more aggressive tendency in younger age groups. In contrast, Veness et al.34 reported that it was difficult to predict prognosis by age35. However, in recent years, the incidence of OSCC is increasing in younger age groups363738.
In overall period, the COP-MPV group A was longer (50.55 months) than the COP-MPV group B (36.64 months) (P=0.019). There was no statistically significant relationship between COP-MPV score and sex, tumor location, N-metastasis, and TNM stage.(Table 1)
Multivariate analysis showed N-metastasis and COP-MPV were statistically significant independent prognostic factors. The N-metastasis group had a 6.227 times higher risk of death than the non-metastasis group (HR 6.227, 95% CI 1.401–27.672) and the risk of death in COP-MPV group B was 18.992 times higher than COP-MPV group A (HR 18.992, 95% CI 1.867–193.212, P=0.013). These results indicate that COP-MPV score had a greater effect on survival prognosis for OSCC patients than N-metastasis.
During the observation period, the survival rate of COP-MPV group B (56%) was significantly lower than that of COP-MPV group A (93.4%). The survival rate of the N-metastasis group was 50% and the survival rate of the non-metastasis group was 76.7%. Kaplan-Meier analysis showed the survival rate in the N-metastasis group was not better than that of the non-metastasis group (Fig. 2), and there was no statistically significant difference in survival rates between the group with maximum tumor size larger than the cut-off value and the group with maximum tumor size not larger than the cut-off value (P=0.365). Zhang et al.39 reported a 5-year survival rate of 20.5% in the N-metastasis group for OSCC patients and 72.3% in the non-metastasis group, claiming that N-metastasis was a more important prognostic factor for predicting survival rate than T stage. Through Cox regression, this study has shown that COP-MPV score (P=0.013) is a more meaningful prognostic factor than N-metastasis (P=0.016) for predicting the survival rate of OSCC patients. These results are similar to those of Zhang et al.40 regarding esophageal squamous cell carcinoma patients.
Khandavilli et al.41 reported that patients with OSCC with high preoperative CRP levels had poor prognosis, and that patients in TNF stage III and IV had relatively higher preoperative CRP levels than patients in stage I and II. Gockel et al.42 reported that lymph node metastasis and tumor extension increased in patients with higher CRP levels, and Park et al.43 reported that survival rate was low in patients with a high CRP/albumin ratio. Similar to these results, CRP (≥0.345 vs <0.345) (P=0.001) was a statistically significant prognostic factor on univariate analysis in this study. However, on multivariate analysis, CRP (P=0.198) was not an independent prognostic factor. These results indicate that the stratifying ability of CRP was likely incorporated in the COP-MPV score.
Kaplan-Meier analysis showed the survival rate of COP-MPV group A was higher than group B indicating that, if both COP and MPV were lower than the cut-off value, postoperative prognosis would be better.
Univariate analysis showed the P-value for PLT was 0.018 and the P-value for MPV was 0.168. PLT was a statistically significant prognostic factor alone but MPV alone was not. However, COP-MPV score (P=0.014) combining PLT and MPV was a more significant prognostic factor than PLT (P=0.018). These results suggest that COP-MPV score, which considers PLT and MPV in a comprehensive manner, is helpful for predicting the prognosis for OSCC patients.
This study has several limitations. First, the sample size is relatively small and it was a retrospective study conducted at a single institution. The initial hypothesis predicted that prognosis would be worse if both COP and MPV were higher than the cut-off value, but it was difficult to confirm this statistically because of the small sample size. Furthermore, the cut-off values for COP and MPV set in this study are not generally applicable to all patients with OSCC. In this study, COP-MPV score had more statistically significant results than other prognostic factors in determining OSCC patient prognosis. Future prospective studies with more subjects using COP-MPV score as a prognostic factor are needed to identify the applicable cut-off value for all patients with OSCC.
V. Conclusion
This study established that COP-MPV score was statistically significant for predicting the prognosis of 40 patients with OSCC. Multivariate analysis showed the survival rate of COP-MPV group B was lower than group A and COP-MPV score (HR 18.992, P=0.013) was found to be a more significant independent prognostic factor than N-metastasis (HR 6.227, P=0.016). COP-MPV score is a simple and cost-effective test method, and is considered a more effective factor relative to other considered factors in predicting OSCC patient prognosis.


 XML Download
XML Download