

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Van der Woude syndrome (VWS) is a rare developmental disorder that is inherited as an autosomal dominant trait with a prevalence of 1 in 75,000 to 1 in 100,000 live births1. The cardinal features of the syndrome include lower lip pits with or without cleft lip or palate.
The most consistent feature is the occurrence of lip pits on the vermilion border of the lower lip, which are seen in nearly 90% of the cases2. Classically, patients present with two bilateral and symmetrical paramedian pits on either side of the midline of the lower lip1234. However, they can also be unilateral, medial, or bilaterally asymmetrical24. A single pit usually represents an incomplete expression of the syndrome3. Rarely, VWS is associated with a number of other findings like hypodontia, ankyloglossia, limb deformities, ankyloblepheron, genitourinary, cardiovascular abnormalities, and popliteal webs2345.
We report a case of VWS in a 10-year-old male with a history of bilateral cleft lip and cleft palate repair, who presented with a single median lower lip pit and associated microstomia, hypodontia, and clubbing of the left foot with syndactyly of the second to fifth lesser toes of the same foot. We could not find any documented cases of median lower lip pits with associated dental, orofacial, and limb deformities, thus adding to the rarity of this case.
The written informed consent was obtained from the patient's guardian.
Go to : 
II. Case Report
A 10-year-old male patient presented to our unit for treatment of a deformity that had been present on the lower lip since birth.(Fig. 1. A) The patient had undergone surgical repair of a bilateral cleft lip and palate at four months and 10 months of life, respectively. The medical and birth histories of the patient were non-contributory. The family history revealed that the patient's brother also had VWS with two bilaterally symmetrical lower lip pits with a cleft lip. On extraoral examination, the patient was found to have a concave profile, suggestive of a hypoplastic maxilla, with microstomia and bilateral scars from the previous lip surgery.(Fig. 1. B) The lower lip deformity was a single, circular, and invaginated midline lesion on the vermilion border, roughly 1.0×1.0 cm in size that was soft and non-tender.(Fig. 1. C) The size of the lesion remained unchanged throughout the patient's life. The lesion also contained a transverse, slit-like opening that, on gentle manipulation of the lower lip, secreted thick mucus. Using a lacrimal probe, the pit was found to have a depth of 17 mm. The patient was examined for associated anomalies, which revealed clubbing of the left foot with syndactyly of the second to fifth lesser toes.(Fig. 2) On intraoral examination, a scar on the soft palate from previous cleft palate repair was present.(Fig. 3. A) Along the maxillary arch, the right central incisor and right and left lateral incisors were found to be missing. On the mandibular arch, the left deciduous second molar was found to be over-retained.(Fig. 3. A, 3. B) On orthopantamogram, the tooth germs of the maxillary right central incisor, the right and left lateral incisors, and the mandibular left second premolar were found to be absent.(Fig. 3. C)
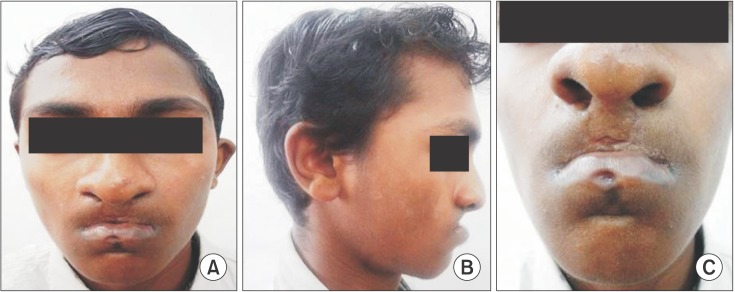 | Fig. 1Preoperative photographs of the patient. A. Frontal view showing the lower lip deformity. B. Profile view demonstrating maxillary hypoplasia. C. Close-up view showing the single median lower lip pit with bilateral scars of previous surgery for cleft palate repair.
|
 | Fig. 2Photograph of the left foot. A. Photograph demonstrating clubbing of the left foot. B. Photograph showing syndactyly of the second to fifth lesser toes of the left foot.
|
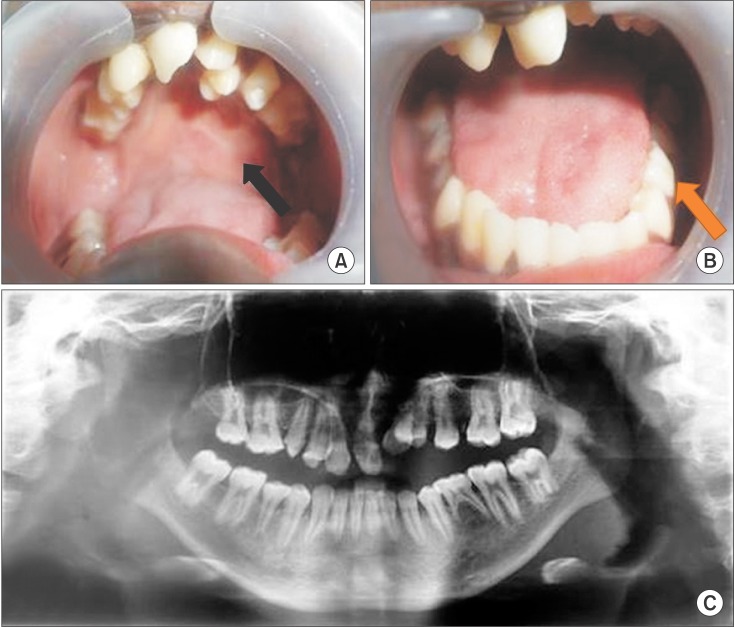 | Fig. 3Intraoral views and orthopantamogram view. A. Photograph demontrating clinically missing maxillary right central incisor and right and left lateral incisors. The palatal scar of previous palatoplasty surgery also evident (arrow). B. Photograph demonstrating overretained mandibular deciduous left second molar (arrow). C. Orthopantamogram showing missing tooth germs of maxillary right central incisor, right and left lateral incisors and of mandibular left second premolar.
|
Following informed written consent, the patient was scheduled for surgical excision of the lip pit under general anesthesia. A vertical wedge excision was carried out for cosmetic reasons.(Fig. 4) Postoperatively, the patient had a cosmetically acceptable scar that was shadowed in the mentolabial sulcus. Both the patient and his parents were highly satisfied with the final surgical outcome.(Fig. 5)


Go to :
III. Discussion
VWS is a rare developmental disorder, yet it is the most common form of orofacial cleft syndrome, accounting for nearly 2% of all cleft lip and palate cases136. Previous attempts at identifying the genes responsible for VWS have not been successful; therefore, no single gene has been implicated as the cause of this condition. In most cases, localization to chromosome 1q32-q41 has been reported; however, localization to chromosome 1p34 has also been seen127.
VWS is an autosomal dominant condition with variable expressivity and penetrance as high as 89% to 99%2. Carriers of the dominant mutation of VWS therefore present as either pits without clefts (44%), pits with clefts (26%), only clefts (10%), or neither clefts nor pits (20%)5.
Lip pits are the most consistent feature of the syndrome and in some cases can be the only manifestation of the syndrome. Approximately 90% of VWS patients display lower lip pits, and in about 64% of cases, lip pits are the only visible defects3. The most accepted theory of lip pit development in VWS involves notching of the lip at the early stage of labial development with fixation of the tissue at the base of the notch5. The other most accepted theory is the persistence of embryonic lateral sulci in the lip following failed fusion, ultimately giving rise to the typical pits seen in VWS8. The surface opening is usually circular, but transverse slits have also been reported. They usually communicate with the underlying minor salivary glands by forming canals that penetrate the orbicularis oris muscle at a variable distance of 1 to 25 mm145. Although the pits are mostly asymptomatic, intermittent to continuous drainage of watery or salivary secretions can sometimes be observed, creating a source of embarrassment for the patient and an unappealing cosmetic problem. Our case displayed a circular pit with a transverse, slit-like opening on the vermilion border of the lower lip. It had a depth of approximately 17 mm and expelled thick mucus on manipulation.
Clefts of the lip and/or palate represent the second most common feature of VWS, seen in nearly 70% of cases1. Of these cases, 50% have a cleft lip and palate, while the other 20% have a cleft palate or submucosal cleft palate. The combination of pits with cleft lip alone is very rare2. The present case was associated with both cleft lip and cleft palate.
Among the associated features seen with lip pits, hypodontia represents the most common anomaly and is observed in 10% to 81% of all patients with VWS358. Although it is a frequently observed anomaly, it might not be obvious at presentation due to the fact that many patients present at a pre-eruption age. Missing incisors or premolars is the most common finding, with hypodontia of the maxillary arch being more common than hypodontia of the mandibular arch58. While the patient in this case presented with hypodontia of both arches, he was missing a greater number of teeth missing in the upper arch than in the lower arch. Other rare anomalies associated with lip pits include ankyloglossia, ankyloblepheron, limb deformities such as hand syndactyly, clubbed feet, tapering fingers, popliteal webs, and genitourinary and cardiovascular anomalies2345. Our case presented with clubbing of the left foot with syndactyly of the second to fifth lesser toes of the same foot.
A considerable phenotypic overlap occurs between the features of VWS and popliteal pterygium syndrome (PPS), as the two disorders affect the same allele. Therefore, patients presenting with lip pits should be evaluated for the presence of PPS. Lip pits are seen in 60 % to 70% of cases with cleft lip and/or palate and popliteal webs4. Anomalies of the genitourinary system, including hypoplastic labia and uteri in females and cryptorchidism and bifid scrota in males, are common findings. Syngnathia and ankyloblepheron filiforme are other craniofacial manifestations of PPS24. Gorlin et al. suggested that the pathognomonic sign for PPS is a triangular overgrowth of the skin over the nail of the first toe2.
The high penetrance of VWS necessitates genetic counselling for family members after careful family history is obtained. Genetic testing typically reveals mutations in the interferon regulatory factor 6 gene, which is considered diagnostic of VWS or PPS and assists in counselling of families with clefts3. In the present case, a positive family history was present. Variants of lower lip pits and clefts, such as submucosal cleft palate, alveolar cleft, or bifid uvula, might be not be apparent to family members, and in such cases, evaluation by photographs or physical examination should be performed4.
The management of VWS is aimed at surgical and esthetic repair of clefts and lip pits3910. A number of techniques have been described in the literature for excising lip pits. They range from simple excision, vertical wedge resection, split lip advancement, and resection with AlloDerm graft implantation to the recently introduced inverted T lip reduction11. All techniques have their inherent advantages and disadvantages, and no single technique can be consistently applied for excision of all lip pits. The nature of the deformity dictates the choice of one technique over the others111. Complete removal of the tract is warranted to prevent the development of mucoceles that would require further surgical intervention411. We selected a vertical wedge resection that helped maintain the regularity of the white roll. The overall outcome was cosmetically acceptable.
In conclusion, we reported a case of VWS presenting with a single median lower lip pit with bilateral cleft lip and palate associated with hypodontia, microstomia, and clubbing of the left foot with syndactyly of the second to fifth lesser toes. Lip pits are the most defined feature of the syndrome, and they occur in almost 90% of cases. Furthermore, in patients with lip pits, thorough history and physical examination are instrumental in diagnosing additional anomalies and distinguishing VWS from PPS. Because VWS has high penetrance, genetic counselling is necessary to identify other family members with the syndrome.
Go to :
 XML Download
XML Download