

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
The concept of natural head position (NHP) was first introduced by Broca1 in 1862, and was described as a stable physiologic position “when a man is standing and his visual axis is horizontal.” In 1958, NHP was described more specifically as “a standardized and reproducible orientation of the head in space when one is focusing on a distant point at eye level”2.
Physiologically, head position is controlled by vestibuloocular and vestibulospinal reflexes, as well as by inner ear otolithic gravitational responses that provide interactions among eye position, head position, and muscles3. According to previous studies, NHP can be influenced by nasorespiratory function456, occlusion789, craniofacial skeletal morphologic features, and visual feedback deprivation10. Based on these findings, NHP might change with emotional state, age, personal characteristics, environmental conditions, and cervical discomfort11.
NHP has been used routinely for clinical examination in medicine and dentistry by plastic and maxillofacial surgeons, as well as by orthodontists. Since NHP provides a coordinate reference system for measurements and therefore has vital importance for orthodontic diagnosis, surgical design, postoperative outcome evaluation, and developmental tracking in patients with dentomaxillofacial deformities, it has drawn the interest of many experts121314.
Previous studies have mainly focused on how to record NHP with two-dimensional (2D) cephalograms1516171819. Unfortunately, traditional methods for recording NHP are limited to 2D cephalograms and are not appropriate for three-dimensional (3D) models. Clinicians use 3D intracranial reference planes in place of 3D NHP models2021.
Now, with the advent of 3D technology, many authors have introduced new methods for recording 3D NHP with cone-beam computed tomography (CBCT) and integrating it into computer-assisted 3D diagnosis and evaluation. However, because patient head position is random during CBCT acquisition, it is difficult to place each person in his or her NHP. To solve this problem, we developed an accelerometer to record patient NHP and reproduce it in CBCT images. We also tested the accuracy and reproducibility of our accelerometer.
II. Materials and Methods
This study was conducted at the Departments of Oral and Maxillofacial Surgery and/or Orthodontics, College of Dentistry, Wonkwang University (Iksan, Korea) from April to October 2016. Fifteen patients (7 males and 8 females; mean age, 25.2 years) participated in this study. Their chief complaint was facial asymmetry. The study was approved by the Institutional Review Board of Wonkwang University (w1410/002-001), and informed consent was obtained prior to patient enrollment.
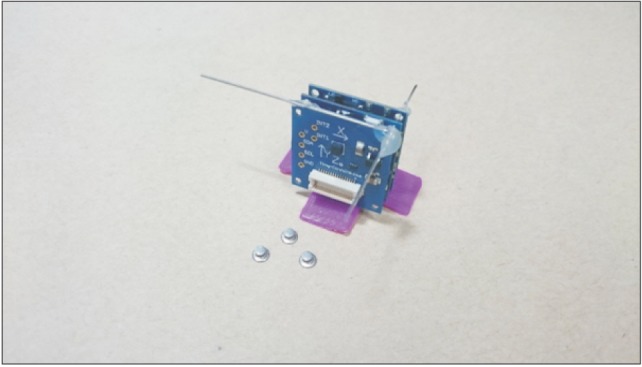
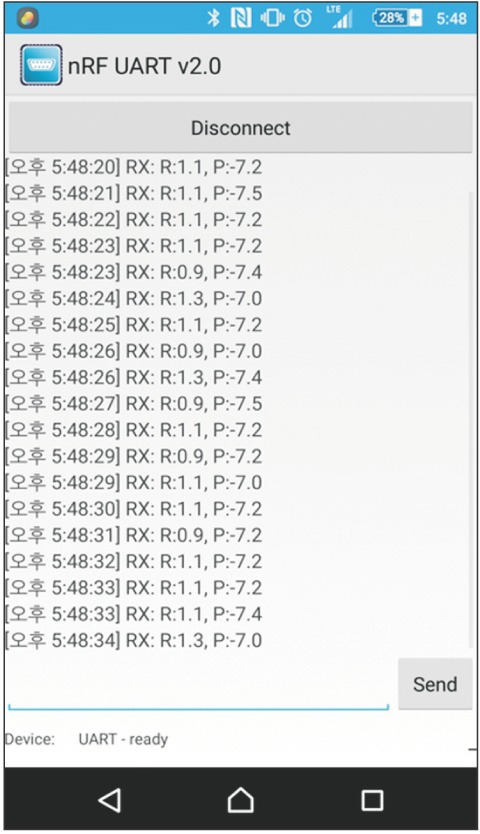
We invented a small accelerometer (3×3×2 cm, 60 g) using the TinyDuino Platform (TinyCircuits, Akron, OH, USA) with a Nordic BLE nRF8001 chip and a Bosch BMA250 chip. The horizontal axis and vertical axis of the device are indicated with 2 wires.(Fig. 1) The Nordic BLE nRF8001 chip enables the device to communicate with the investigator's smartphone through an application (nRF UART v2.0) using Bluetooth technology (ver. 4.0. Bosch BMA250 chip). The accelerometer has the following characteristics—digital resolution: 10 bits; measurement ranges: ±2 g, ±4 g, ±8 g, ±16 g; sensitivity: 2 g: 256 LSB/g, 4 g: 128 LSB/g, 8 g: 64 LSB/g, 16 g: 32 LSB/g, zero-g offset (over lifetime): ±80 mg measures 3-axis acceleration, and roll and pitch are calculated every 0.5 seconds using an inverse trigonometric function. The last five data points in the average were used as the patient NHP (roll and pitch).(Fig. 2)
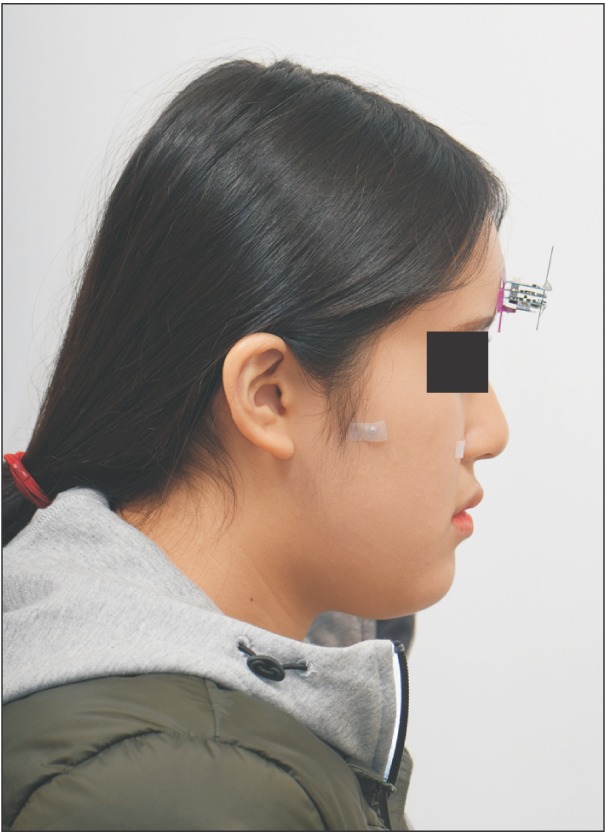
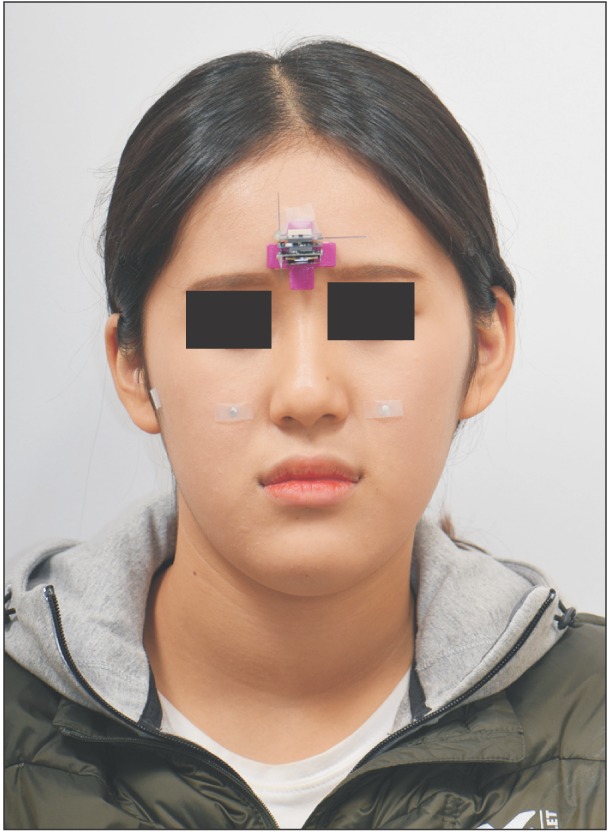
The device was attached to each subject's forehead with skin tape, and three lingual buttons were placed in the preauricular area and on both zygomatic areas.(Fig. 3, 4) Subject NHP (roll and pitch) was recorded using a mirror-guided technique.(Fig. 5) Frontal and lateral clinical photos were taken, and then a CBCT with a standard Frankfort horizontal (F-H) plane-based position was taken.
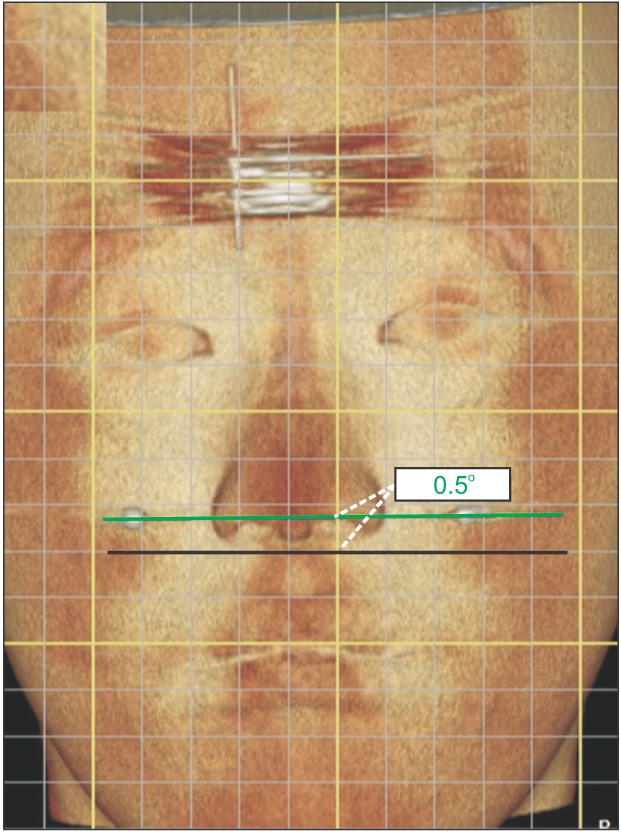
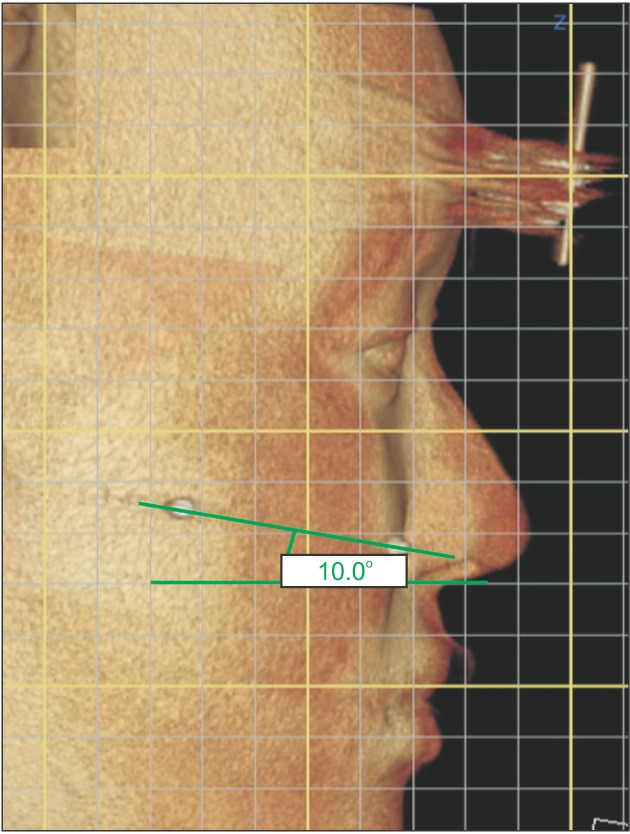
Those CT data were reconstructed with OnDemand3D ver. 1.0 (Cybermed Inc., Tustin, CA, USA), and reorientation was performed using the device's horizontal and vertical axes. (Fig. 6) Recorded NHP roll and pitch data were applied to the reoriented virtual image. On the virtually recreated NHP 3D model, we made a line between two lingual buttons present on each the frontal and lateral side. The angles between those lines and the horizontal line were calculated.(Fig. 7, 8) The same procedure was conducted on the clinical photos. These angles between the 3D models and the clinical photos were statistically analyzed side by side.
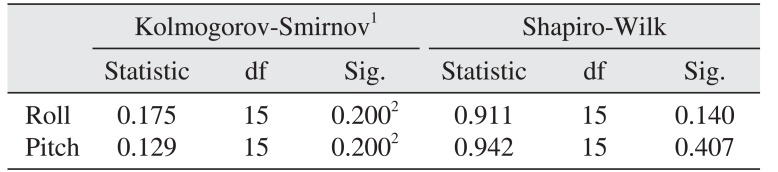
The Kolmogorov-Smirnov test and the Shapiro-Wilk test were used to test for normality. The comparisons of the angles between the 3D models and the clinical photos were conducted with paired t-tests. IBM SPSS ver. 21.0 for Windows (IBM Co., Armonk, NY, USA) was used for all analysis. A two-tailed P-value <0.05 was considered statistically significant for all analyses.
III. Results
The average difference between the angle in the clinical photograph and the angle in the 3D model was 0.04° for the roll and 0.29° for the pitch. Both roll and pitch data were normally distributed, according to the Kolmogorov-Smirnov test and the Shapiro-Wilk test.(Table 1)
The results from the paired t-tests for the roll data (P=0.781) and the pitch data (P=0.169) indicated that there was no significant difference between the clinical photographs and the 3D model (P>0.05).(Table 2)
IV. Discussion
In this study, we used the mirror position technique to acquire patient NHP. Three methods have been widely used to acquire NHP; the self-balanced position, the mirror position, and the estimated position. The self-balanced position asks the patient to look into horizontal infinity12, and the mirror position asks the patient to look into his or her own eyes in a mirror322. The estimated position is generally thought to be that wherein the head position can be reproduced with less variation when corrections are made by the doctor2. A study that investigated the reproducibility of the roll and pitch of NHP found no significant differences in those three methods in reproducibility for either measure23.
Recording patient NHP and reproducing it in a virtual environment is becoming increasingly important for pretreatment planning and posttreatment evaluation. One of the most common methods for orienting a 3D CT model in NHP is to use the clinician's insight or digitized landmarks to the NHP24. This method is more accurate when the craniofacial structures are symmetrical than when the patient has severe facial asymmetries. Recently, several newly developed methods for recording NHP in three dimensions have been introduced, including a digital gyroscope that can record NHP in three dimensions1225. For this method, an electronic device is mounted on a bite jig, and the patient holds the device by biting the bite jig until the 3D photographs are taken with the patient in a NHP. The NHP orientation data are automatically recorded and transferred to the virtual imaging software for 3D CT model reconstruction. However, there is potential for error because the patient is holding a heavy instrument for a long period of time12. The 3dMDface imaging system was used to record sitting NHP32627. For this method, four ink dots were marked on a patient's face to record NHP before taking the 3D photograph. However, because the patient's head is prone to moving while dots are marked on the face, this technique is not reliable.
To overcome those difficulties, we developed a new method to record NHP and to transfer the NHP to the 3D CT model. NHP recording methods should not influence head orientation. We designed an accelerometer that is not only smaller (3×3×2 cm), but also lighter (60 g) than any other previous devices. We placed the device on the patient's forehead so that its center of gravity aligned with that of the patient's head. Also, as long as the device was placed on the patient's head, its specific position was not a concern. Because we wanted to assess the device's accuracy in reproducing each patient's individual NHP in 3D images, the device was attached to each patient's forehead and did not move until the clinical photo and CBCT were taken. Because the device can calculate real-time roll and pitch angles (per 0.5 seconds) and record those data automatically, there is no time interval between acquiring and recording NHP. In this study, a clinician attached the device to a patient before taking clinical photographs, so this procedure itself does not affect NHP acquisition or recording. Since it does not require additional devices or procedures, we could record patient NHP at the first visit within a few seconds while clinical photographs were taken. Furthermore, it is possible to reconstruct individual NHP on any diagnostic software that supports coordinate-dependent modeling. Reconstructed NHP on a 3D simulator showed no significant differences (P>0.005) in NHP; all differences (average differences were 0.04° in roll and 0.29° in pitch) were within the established NHP variability of 2°228. However, the small number of patients (n=15) was a limitation of this study. Also, we did not identify NHP yawing, which is a very important factor for diagnosing facial asymmetry, as analyzing data with only pitch and roll can lead to errors in the estimated position in 3D space. In future studies, more patients and yaw analysis should be included. All of our procedures were conducted by one examiner.



 XML Download
XML Download