

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Sialolithiasis, the most common salivary gland pathology, is caused by calculi in the gland itself and its duct1. Gland swelling and pain are the chief complaints of presenting patients23. Most salivary gland calculi occur in the submandibular gland (83%), followed by the parotid (10%), sublingual and minor salivary glands (7%)4. Calculus size varies from less than 1 mm to a few centimeters5. Most salivary calculi are smaller than 10 mm; giant ones, larger than 15 mm and occurring only rarely, are known as sialoliths26.
While patients with small sialoliths can undergo conservative treatment, those with standard-size or larger sialoliths require sialolithotomy578. Most submandibular calculi, located in the distal third of the duct, are removed surgically via direct incision to the stone5791011. This procedure is relatively simple to perform, and does not often result in complications10. Sialoliths that are sufficiently small and near the duct orifice can be manipulated and removed. Another minimally invasive method is using sialogogues with gland massage to promote salivation and flush the small sialoliths to the duct orifice7812. Carelessness during this treatment, however, can cause rupture of the duct12.
In the present case study, we removed two sialoliths located beneath the mucosa in the posterior and anterior regions of Wharton's duct, respectively. For the posterior calculus, we performed a sialolithotomy via an intra-oral approach; thereafter, the small anterior calculus near the duct orifice was removed by hydraulic power. Postoperatively, the patient's symptoms disappeared, and there have been no complications since.
Go to : 
II. Case Report
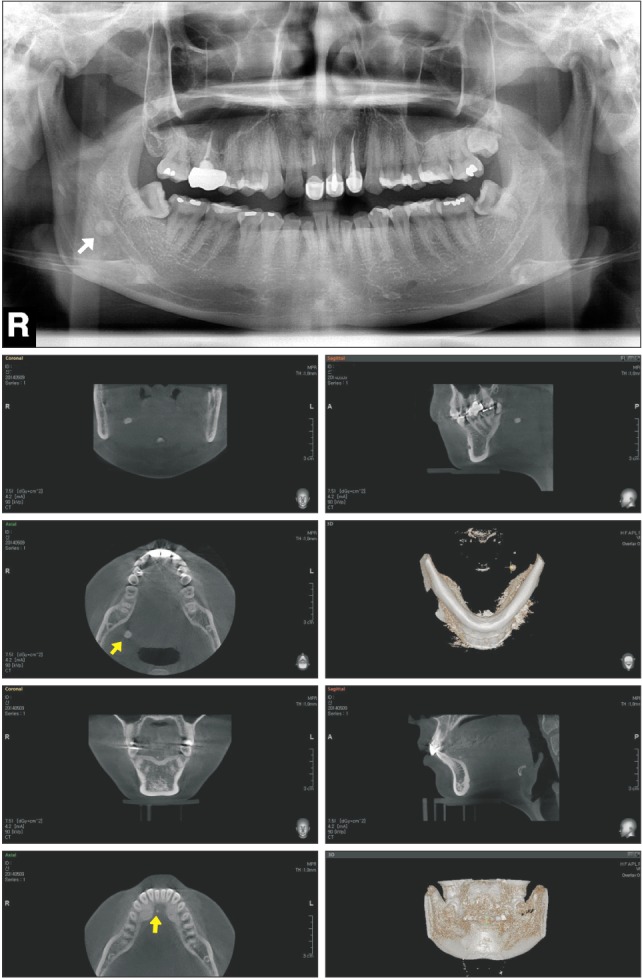
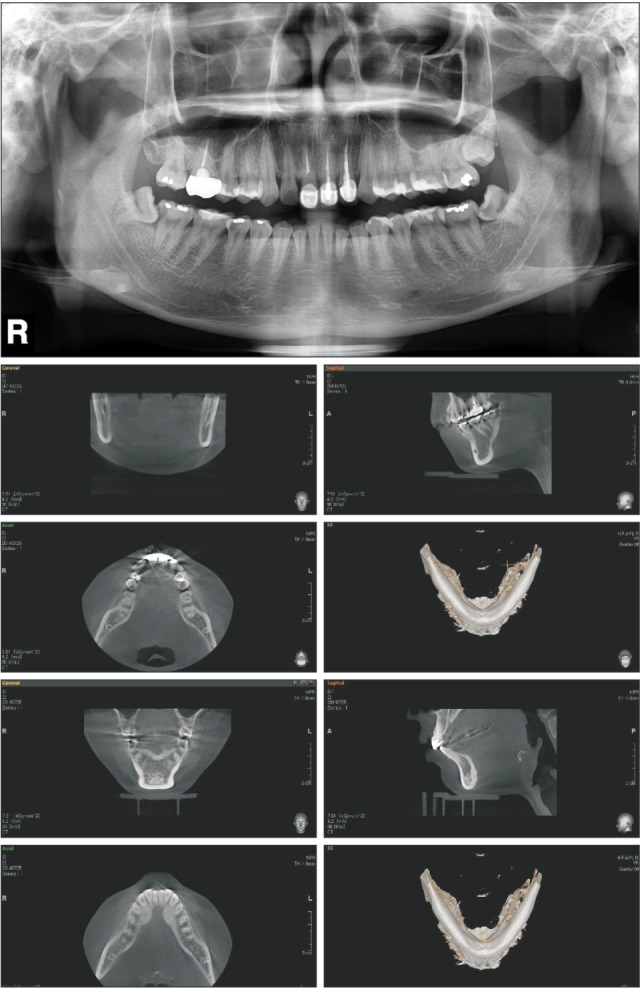
A 21-year-old female patient presented with a chief complaint of a firm mass on the right side of the floor of the mouth and uncomfortable swallowing for the preceding 4 months. She had no pain, fever, chills or lymph node swelling. Intra-oral examination by bimanual palpation revealed a small, firm, and non-tender swelling of the anterior floor of the mouth as well as a large, firm and non-tender swelling in the region opposite #38. Panoramic radiography and cone-beam computed tomography confirmed two calcified lesions in the posterior and anterior regions of the right Wharton's duct, respectively.(Fig. 1) The final diagnosis was sialolithiasis in the right Wharton's duct.
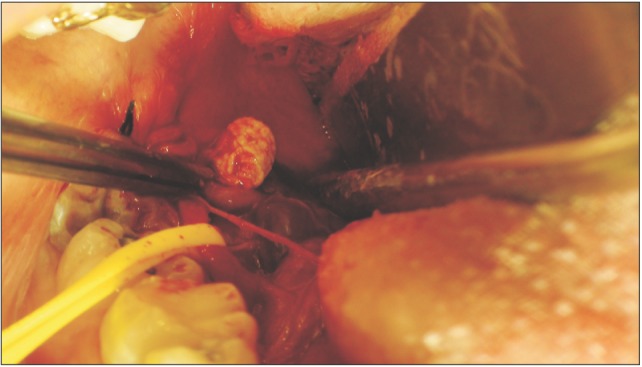
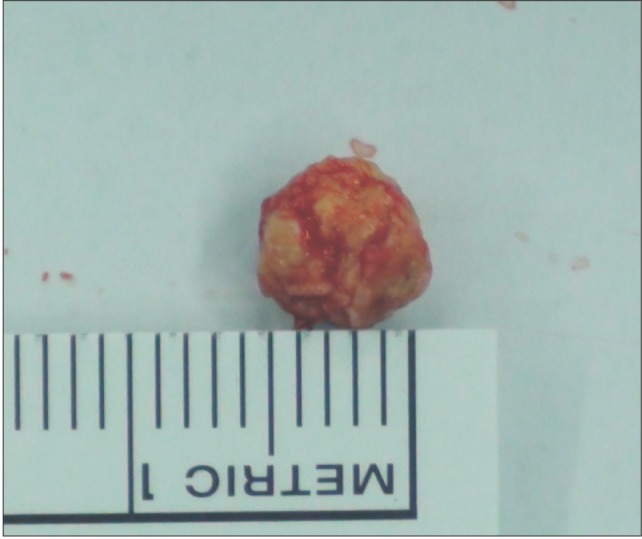
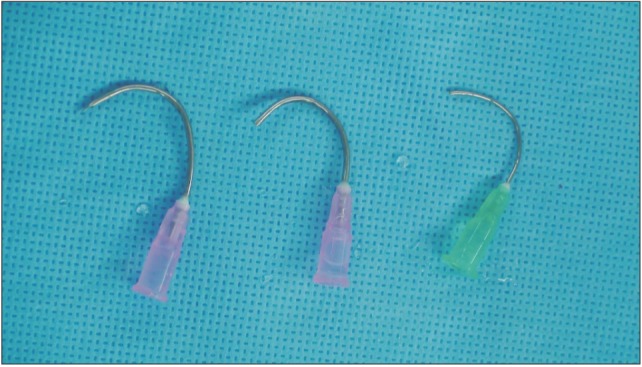
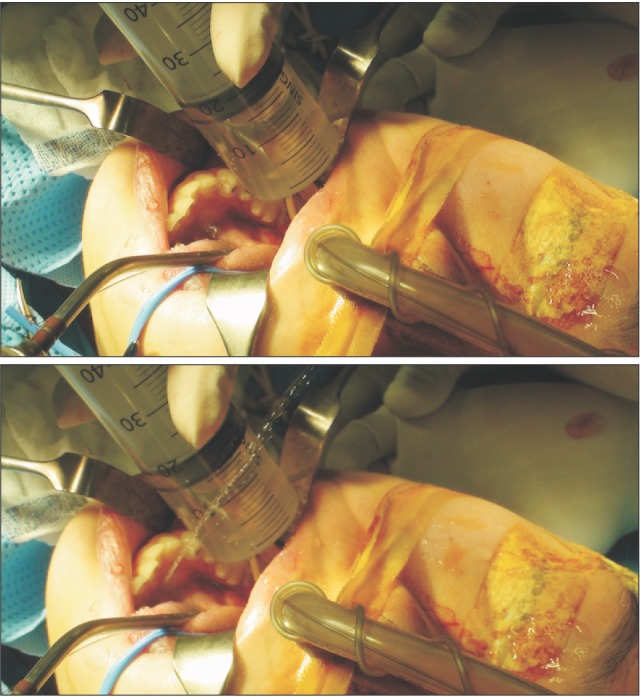
The posterior sialolith was removed intra-orally by sialolithotomy under general anesthesia, incising directly to the stone along the longitudinal axis of the duct and cautiously avoiding the nearby lingual nerve.(Fig. 2) The duct, which was 6 mm in diameter (Fig. 3), was left open, enabling successful, complication-free removal of the anterior sialolith by hydraulic power using a 50-mL syringe with a curved 18-gauge needle.(Fig. 4, 5) After inserting the needle into the open duct, the syringe was used to spout saline water to flush the small sialolith. Based on the saline that came from the duct orifice, we checked that the front of the sialolith was removed. The postoperative radiography was clear, indicating no remaining sialoliths. After one week and then again at two months, the patient was reviewed to assess gland's salivary function, which proved normal.(Fig. 6) To date, after 2 years, the patient has been asymptomatic, showing no recurrence.
Go to :
III. Discussion
Sialolithiasis is the most common pathology of the salivary glands1. The precise pathogenesis is still mostly unknown; however, for treatment of sialolithiasis of the Wharton's duct, there are various methods available, the selection of which depends on the calculi location and size as well as the likelihood of complications based on careful consideration of the patient's specific condition and symptoms121314.
The available methods range from conservative management to surgery5. The non-invasive options include hydration of the patient, prescription of sialogogues, and gland massage, all of which can be helpful in promoting salivation and consequent flushing of the calculus712. As for minimally invasive treatment, manipulation using lacrimal probes and dilators to open the duct orifice is useful in order to milk the calculus, manipulate it forward, and then remove it7. The invasive, surgical approach entails incision along the longitudinal axis of the Wharton's duct directly onto the stone, most of which are submandibular calculi located in the duct's distalthird region78.
This paper presents a case report of a patient with two sialoliths in the right Wharton's duct. One sialolith, located posteriorly in the distal third of the duct, was surgically excised by sialolithotomy, after which the other, located anteriorly near the orifice, was removed through the duct by hydraulic power. The former surgical method is required to remove large stones in the back of the duct. Then, the least invasive method possible should be used for removal of any stones blocking the duct that are smaller than the diameter of the duct. Careless use of a lacrimal probe is likely to result in rupture of the duct, so we needed a new, easier and safer approach. We chose to try hydraulic power because it is less invasive than a lacrimal probe.
The use of hydraulic power is limited in that it requires another incision and the diameter of the stone should be less than the diameter of the duct. Removal of only a small stone, located anteriorly near the orifice, can be achieved with conventional methods. Our future work will focus on determining indications for the use of hydraulic power method for less invasive removal of sialoliths.
This method has not been reported previously. There were no complications either during the operation or postoperatively, and the salivary function of the gland remained normal.
Go to :
 XML Download
XML Download