

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Bisphosphonate is the most widely used therapeutic agent for osteoporosis in South Korea. It has been in the spotlight over the last few years as a therapeutic agent for metabolic disease, spinal cord compression, pathologic fractures, pain, etc123. It is known that a certain amount of bisphosphonate administered systemically is absorbed by the bone tissue, and that the rest is discharged through the kidneys45. Bisphosphonate is discharged through 3 pathways: (1) glomerular filtration rate (GFR); (2) renal tubular secretion; and reabsorption within the renal tubular lumen456. The excretion of bisphosphonate is closely associated with the renal clearance rate6 and is thought to be closely tied to the patient's renal function or systemic diseases that are affecting renal function7.(Fig. 1)
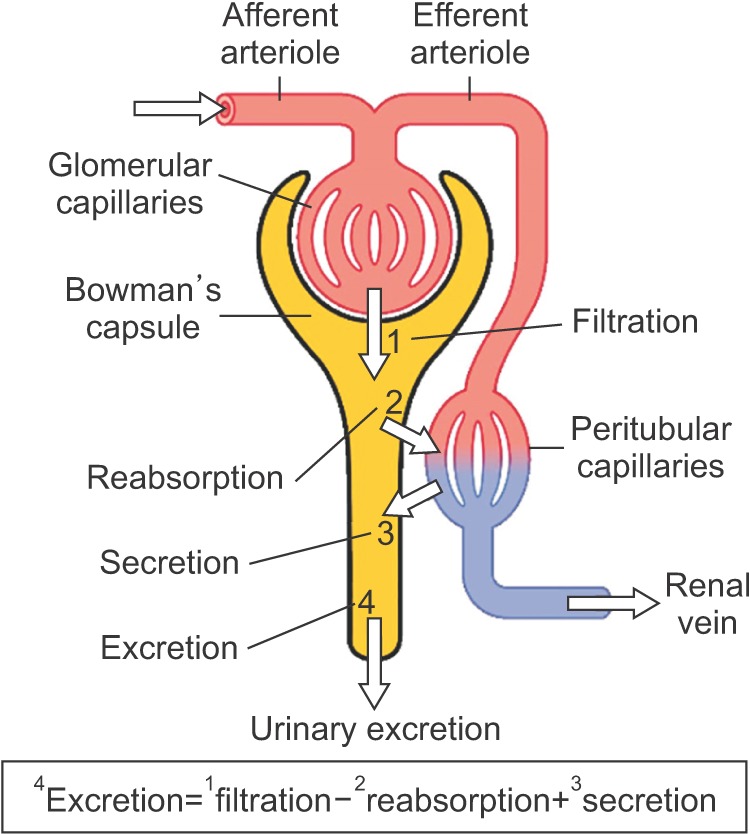 | Fig. 1Renal excretion. Adapted from the Wikipedia: Renal function7.
|
Since Marx8 first reported bisphosphonate-related osteonecrosis of the jaw (BRONJ) in 2003, it has been the topic of many studies. In the 2009 position paper of the American Association of Oral and Maxillofacial Surgeons (AAOMS), BRONJ was defined according to the following criteria: (1) past or current bisphosphonate therapy history; (2) exposed necrotic bone present in the jaw area, present for more than 8 weeks; and (3) no radiation therapy in the jaw. Below are the detailed criteria for staging9.(Table 1)

Table 1
Staging system of the American Association of Oral and Maxillofacial Surgeons for BRONJ9
![]()
Silva et al.10 reported that the incidence of BRONJ increased when more than a certain level of zoledronate was administered. In a study conducted by Manzano-Moreno et al.11, as the duration of bisphosphonate administration increased, the differentiation of the osteoblast-like cells decreased, and cell death and necrosis occurred. The bisphosphonate deposited in the bone is isolated only if the bone is re-absorbed, and the half-life is about 10 years6. Therefore, as the duration of bisphosphonate treatment increases, the concentration of deposited bisphosphonate increases. Moreover, as the patient's renal function decreases, the deposition of bisphosphonate will increase. Thus, BRONJ is expected to become more severe.
The purpose of this study was to identify the relationship between severity of BRONJ and renal function by comparing the results of the clinical tests, radiological examinations, serologic tests, and medical records of patients assessed for BRONJ. Renal function was assessed based on the criteria of the National Kidney Foundation (NKF) and International Society of Nephrology (ISN)1213.(Table 2) Through this investigation, we intended to identify the factors that significantly affect the severity of each group.

Table 2
CKD: a clinical action plan
![]()
Go to : 
II. Materials and Methods
1. Subjects
In this study, we analyzed 106 patients who had been diagnosed with BRONJ through clinical tests and radiography and who had been treated at the Department of Oral and Maxillofacial Surgery of the Pusan National University Dental Hospital (Yangsan, Korea) within the period from January 2012 to December 2014. Of these patients, 13 had an ambiguous bisphosphonate formulation component or had discontinued regular follow-up. For the ramining 93 patients, the type of bisphosphonate administered, the duration of its administration, drug holiday timing, administration route, and presence of systemic diseases were examined through clinical tests and medical history. In addition, the following serologic tests were performed liver function test (LFT), renal function test (RFT), electrolyte test, C-reactive protein (CRP) test, HbA1c test, and C-telopeptide crosslink (CTX) test. For radiological examination, panoramic radiography and cone-beam computed tomography were conducted.
The study was approved by the Institutional Review Board of the Pusan National University Dental Hospital (PNUDH-2016-007).
2. Methods
For all patients, the medical history and serologic test results were recorded, and the panoramic radiography and cone-beam computed tomography, which were performed at the initial examination, were analyzed. The presence of an exposed bone determined through visual inspection and palpation, the finding of an infection, the size of the lesion, and the clinical symptoms were classified. The stage of BRONJ was based on the 2009 AAOMS position paper9 (Table 1) and was determined based on the analyzed medical records and radiographic images. The systemic diseases that can affect the renal function of the patients were roughly classified into heart disease, diabetes, liver disease, thyroid disease, and kidney disease. For arithmetic evaluation, the estimated glomerular filtration rate (eGFR) was calculated based on the CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) creatinine equation (2009)14, and the CKD stage was also determined based on the calculated eGFR value12.
Through consultation with physicians, 91 patients had an average drug holiday lasting 15.0 weeks before surgery. A total of 46 patients (50.5%) had a less-than-1-month drug holiday, and 20 patients (22.0%) had a 1- to 3-month drug holiday. A total of 25 patients (27.5%) had a more-than-3-month drug holiday, as suggested in the 2009 AAOMS position paper. After the surgery, all 93 patients stopped taking bisphosphonate915.
As in our previous study conducted by Park et al.15, after the drug holiday, for the stage 1 patients, conservative treatment was administered; for the stage 2 patients, sequestrectomy and curettage of soft tissue were performed; and for the stage 3 patients, including sequestrectomy and curettage of soft tissue, fistula closure, mandibulectomy, or mandibular reconstruction was performed. For the conservative treatment, antibiotic treatments were administered, along with oral cleaning using a sanitizer (0.12% chlorhexidine), as suggested in the treatment strategy cited in the 2009 AAOMS position paper. For the antibiotic, penicillin was selected as the first-choice medication. Oral hygiene instruction was also offered, and follow-up examination was conducted every 2 weeks.
Evaluation of each group for prognosis was conducted 6 months after the start of treatment. For evaluation, if pain, infection, re-exposure of the bone necrosis site, and fistula formation were not observed and the patients showed a good treatment prognosis, the patient was assigned to the responder group. If no clinical and radiological differences were shown before or after the treatment or if BRONJ recurred, the patient was assigned to the non-responder group. If the clinical symptoms (pain, extraoral fistula, pathological fractures, etc.) became worse, the patient was assigned to the worsened group15.
Regression analysis was performed at a 0.05% significance level for the BRONJ stage and the significant serologic markers. All statistical analyses were performed using the IBM SPSS Statistics version 21.0 (IBM Co., Armonk, NY, USA).
Go to :
III. Results
Of the 93 patients, 1 was male and 92 were female. Based on the AAOMS diagnosis criteria, there were 15 patients at stage 1, 53 patients at stage 2, 25 patients at stage 3, and no patient at stage 0. The mean age was 73.2 years (range, 51-86 years). As for the type of bisphosphonate that was administered, alendronate was administered to 54 patients (58.1%), risedronate to 15 patients (16.1%), ibandronate to 17 patients (18.3%), pamidronate to 4 patients (4.3%), and zoledronate to 3 patients (3.2%). For the administration route, 80 patients (86.0%) had oral administration and 13 patients (14.0%) had intravenous administration. The average duration of administration was 5.5 years (range, 0.25-20 years). The mean eGFR calculated using the CKD-EPI creatinine equation was 65.9 mL/min/1.73 m2. The 83 patients who responded during the 6 months after treatment were assigned to the responder group, the 5 patients who did not respond to the treatment were assigned to the non-responder group, and 5 patients were assigned to the worsened group.
To determine the correlations between BRONJ stage and the impact factors, regression analysis was used. Among all impact factors, age and eGFR were observed to have a significant correlation with BRONJ stage. In particular, we focused on blood creatine level, which is the representative measure of kidney function. As the severity of BRONJ increased, the patient's creatinine level increased, but the change was not statistically significant.(Tables 3, 4)

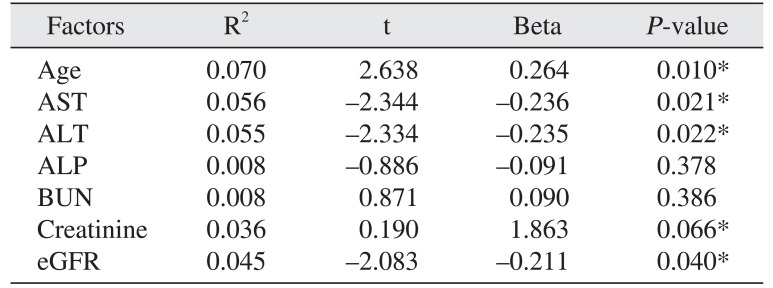
Table 3
The mean values of several impact factors of BRONJ by stage
![]()
Table 4
The results of regression analysis for several impact factors with BRONJ stage
![]()
There was no definite effect of serum calcium level, serum albumin level, type of bisphosphonate, route of administration, duration of medication or drug holiday, presence of a systemic disease, or CTX level on BRONJ stage.
To determine the correlation between the degree of response to treatment and BRONJ stage, the patients were assigned to the responder, non-responder, or worsened group. The responder group showed a lower BRONJ stage compared to the non-responder group, and this difference was statistically significant.(Table 5)

Go to :
IV. Discussion
Bisphosphonate is one of the most widely prescribed drugs for patients with osteoporosis. It increases the bone density by depositing serum calcium in the bone, reduces the bone turnover rate, and decreases the risk of pathologic fracture. As bisphosphonate is generally excreted through the kidneys; however, if an excessively high plasma level is maintained, it may have a side effect on the kidneys5. The incidences of osteoporosis and kidney failure are both known to increase with aging1617. Considering this, the relationship between BRONJ and renal function needs to be addressed.
BRONJ was first published in the 2007 AAOMS position paper18, and the criteria for its stage and drug holiday were suggested in the 2009 position paper9. Moreover, in 2014, AAOMS published its third position paper on this disease19. In the paper, the definition of BRONJ was changed to “necrosis of the jaw” due to the administration of anti-absorption drugs, anti-angiogenic therapy, etc., as well as bisphosphonate administration, and it was renamed “medication-related osteonecrosis of the jaw (MRONJ)”. As such drugs also go through the kidneys' excretion process, a healthy renal function is considered important in the pharmacokinetic aspect based on the drug concentration.
In the kidney disease: Improving the Global Outcome (KDIGO) group of NKF and ISN, if the eGFR is less than 60 mL/min/1.73 m2 for more than 3 months, regardless of the reason, and if proof of renal damage is found in the blood, urine, radiography, or pathologic examination, the case is defined as CKD (Chronic Kidney Disease)1213. In addition, stage 1-5 CKD is defined according to the eGFR, and guidelines necessary for each stage are proposed1213.(Table 2) In this paper, our patients were classified based on the KDIGO guidelines. Although the eGFR of the patient group could not be followed for 3 months, the study was conducted assuming that all patients had CKD due to the advanced ages (73.2 years on average), based on the study results obtained by O'Hare et al.20 and Gifre et al.21.
The results of the regression analysis showed that the BRONJ stage was significantly correlated with patient age, eGFR, aspartate aminotransferase (AST), alanine aminotransferase (ALT), and the degree of response to treatment. There was not a significant correlation with serum calcium level, serum albumin level, type of bisphosphonate administered, duration of administration, drug holiday period, administration route, presence of a systemic disease, or CTX level.
In terms of AST and ALT, there was a negative correlation, in that BRONJ stage was lower in patients with liver disease with higher AST or ALT. This may have been a problem with our sample group, but it was not considered to be clinically significant.
In general, the factor that is considered to have a great effect on the severity of BRONJ is the efficacy of the bisphosphonate. According to the relevant literature, as the efficiency strength of bisphosphonate increases and the administration duration becomes longer, the incidence of BRONJ increases. Moreover, a higher BRONJ incidence has been observed among patients using injectable bisphosphonates compared to those taking oral bisphosphonates9222324. In this study, the BRONJ stage was not significantly associated with the type of bisphosphonate administered, the duration of administration, or the administration route. This means that the nature of the drug itself or its administration method can increase the incidence of BRONJ, but once BRONJ occurs, the effects of the aforementioned factors on the severity of the disease are not significant. These results suggest that even short-term administration of bisphosphonate formulation can cause progression to severe BRONJ.
In the 2009 AAOMS position paper including guidelines for drug holiday period before surgical treatment, discontinuation of bisphosphonate administration for 3 months before and after the surgery, respectively, was suggested. The study conducted by Damm and Jones25 and published in 2013 also proposed that a 2-month drug holiday period is necessary for the complete excretion of serum bisphosphonate through the kidneys and for the full recovery of the activity of the osteoclasts. On the other hand, the 2014 AAOMS position paper stated that the scientific evidence for the need to discontinue bisphosphonate administration was not sufficient. In this study, no statistical association was found between the BRONJ stage and the washout period, but the BRONJ stage was found to be correlated with the number of patients in both the responder and non-responder groups.
In the study, the responder group showed the lowest mean BRONJ stage, with generally low BRONJ stages. Based on this, we concluded that the severity of BRONJ may not decrease despite a long drug holiday period, and that the probability of responding to the treatment may be low.
The fact, the non-responder group showed the highest mean BRONJ stage, and the distribution of higher BRONJ stages runs counter to the hypothesis of this study. Such a result may be due to the small number of patients in both the non-responder and worsened groups (5 patients, respectively). To establish clear criteria for further guideline, a long-term study based on a large sample size is necessary.
In the study conducted by Marx et al.26, the patients were assigned to the high-risk group if their serum CTX level was less than 100 pg/mL, to the moderate-risk group if their serum CTX level was 100-150 pg/mL, and to the low-risk group if their serum CTX level was higher than 150 pg/mL. In the study conducted by Song et al.27, however, the value obtained through the risk assessment using the CTX level did not have a significant correlation with the severity of BRONJ. Grbic et al.28 reported that the association of CTX level with BRONJ was not sufficient in their study, although a low CTX level was maintained through the long-term administration of zoledronic acid. It was also found in our study that CTX was not significantly correlated with the BRONJ stage.
Patient age is closely associated with the development of BRONJ as well as with renal function. The 2009 AAOMS position paper9 stated that the use of steroids due to another disease or the risk of osteoporosis due to menopause or aging might increase. According to Park et al.29, Bamias et al.30, and Hoff et al.31, the physiological effect of aging seems to be associated with BRONJ. In this study, age and decreased renal function were confounding factors, but occuring result of BRONJ also was obtained when analyzing each of the two factors separately.
On the other hand, Baqain et al.32 and Vahtsevanos et al.33 reported no statistically significant correlation between aging and BRONJ stage. In the present study, patient age did show a statistically significant association with the BRONJ stage.
A typical method of evaluating renal function is calculating the GFR, which can be simply estimated using the creatinine value. With regard to the relationship between the kidneys and bisphosphonate, Markowitz et al.3435 reported that kidney failure occurred in the patients in their study after injection of bisphosphonate, but Gifre et al.21 reported that kidney failure occurred in only 10% of the patients who received bisphosphonate for at least 1 year.
According to Suresh et al.36, in patients with higher than stage 4 CKD, the bisphosphonate administration dose must be reduced or the drug should not be prescribed at all, and in patients with lower than stage 3 CKD, the same dose as that for the general population can be prescribed. According to the aforementioned literature, the incidence of kidney failure due to bisphosphonate administration is higher in patients with lowered renal function, and as such, high-dose bisphosphonate can easily accumulate in the body. Moreover, due to the high-dose bisphosphonate deposit, the probability of kidney failure recurrence increases, and the cycle is repeated. In our study, the BRONJ stage was significantly associated with eGFR. As the CKD stage was also determined according to the eGFR value, CKD would also be associated. Therefore, as the renal function remarkably decreases, CKD stage is higher, and the severity of BRONJ might increase.(Table 2) In addition, we conclude that, as the severity of BRONJ increases, the patient's response to the treatment decreases. (Table 5) Taken together, our results suggest that decreased renal function will result in decreased patient response to the treatment.
In general, the systemic diseases that affect the renal function of patients are hypertension, diabetes, glomerulonephritis, infection, and steroid treatment for osteoarthritis management37. In this study, however, heart disease, diabetes, liver disease, thyroid disease, and kidney disease were found not to have a statistically significant correlation with the BRONJ stage. This was illustrated by a case where the patient was unaware they had an aforementioned disease until diagnosed through clinical and serologic tests, and by a case where the patient did not have any of the aforementioned diseases but was taking a drug for preventive purposes. Additionally, there were cases with no detailed diagnosis, where the patient was completely cured after the surgery, continued to receive the drug and was not examined, or the duration of drug administration or treatment was not calculated. For significant results, more specific variables must be applied for each item. For the aforementioned items, long-term prognosis assessment and follow-up observation targeting a large number of patients are required, and the specifications of renal function and systemic disease will be necessary.
Go to :
V. Conclusion
This study was conducted in 93 patients who had been diagnosed with BRONJ through clinical tests, radiography, and serologic tests at the Department of Oral and Maxillofacial Surgery of Pusan National University Dental Hospital from January 2012 to December 2014. This study aimed to identify the relationship between severity of BRONJ and renal function and to determine the factors that affect this relationship.
The BRONJ stage showed a significant correlation with the renal function value, the eGFR. In addition, the BRONJ stage was found to be significantly correlated with the responder and non-responder groups, but was not significantly correlated with the worsened group. Moreover, the BRONJ stage was found to be significantly correlated with patient age. Therefore, based on the results of our study, we conclude that old patients with remarkably lowered renal function are likely to have more severe BRONJ, and the degree of patient response to the treatment is likely to be low.
Go to :
 XML Download
XML Download