

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Oral cancer is the sixth most common cancer, and its incidence is currently increasing worldwide12. Squamous cell carcinoma (SCCa) of mouth area accounts for more than 90% of all malignant neoplasms in the oral area34. Tongue is the most common site of primary SCCa of the mouth area5.
The most important prognosticator of survival in tongue SCCa is the presence of lymph node metastasis678. In tongue SCCa, the incidence of occult neck metastasis is relatively high; 7%-28% of patients with T1 and 28%-40% of T2 SCCa of the tongue were clinically staged as N0191011. Another study showed the incidence of occult neck metastasis in T1 as 13%-33% and 37%-53% in T212131415. Occult metastasis in T1 is much less frequent than that in T2. The effectiveness of elective neck dissection in patients with clinically negative lymph node (N0) in stage I or II (early) SCCa of the tongue remains controversial112151617181920.
We retrospectively compared the results of elective neck dissection with observation in the treatment of early clinically negative neck in tongue SCCa. We also attempted to evaluate whether elective neck dissection can increase survival time and estimate the value of elective neck dissection in clinically stage I or II tongue SCCa.
II. Materials and Methods
Patients with stage I or stage II SCCa of the tongue who were treated surgically in the Department of Oral and Maxillofacial Surgery, Seoul National University Dental Hospital (Seoul, Korea) between January 2005 and May 2014 were reviewed. All patients had preoperative clinically N0 status and had undergone partial glossectomy with or without elective neck dissection as part of the primary surgical treatment. Patients who had non-SCCa and received radiotherapy or chemotherapy after surgical treatment were excluded. Staging was evaluated according to the 2010 American Joint Committee on Cancer (AJCC) criteria. All patients were staged N0 after clinical and laboratory assessment and preoperative diagnostic examination including palpation and imaging of the neck such as computed tomography, ultrasonography, and magnetic resonance imaging. This study was reviewed by the Institutional Review Board of Seoul National University School of Dentistry (IRB No. S-D20160012).
The patients were divided into two groups according to management of the neck node. The patients in the partial glossectomy without elective neck dissection group had not received any kind of neck treatment. The elective neck dissection group consisted of patients who had undergone prophylactic neck dissection.
The two groups were compared with respect to overall survival (OS) and disease-free survival (DFS). OS was time between the date of first visit to the date of last follow-up or death from any cause. DFS was time from the date of first visit to the date of recurrence. Patients lost to follow-up were included in all analyses, until the date of last follow-up.
All data for statistical analysis were compiled using the IBM SPSS Statistics for Windows (version 21.0; IBM Co., Armonk, NY, USA). Survival curves were plotted using the Kaplan-Meier method and compared using the log-rank test. Cox regression analysis was performed for multi-variance analysis. Statistical significance was indicated by P<0.05.
III. Results
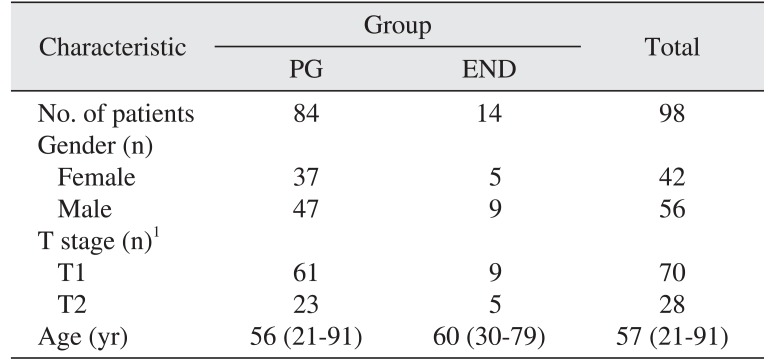
The 98 patients comprised 56 male and 42 female. Patient age ranged from 21 to 91 years with a mean of 57 years, and the mean postoperative follow-up period was 33.7 months. The clinical TNM stage was T1N0M0 in 70 patients and T2N0M0 in 28 patients. All patients were staged N0 by clinical and radiologic assessment.
The most common primary location was the lateral tongue border (70 patients), followed by ventral side (20 patients), dorsal side (6 patients), and tip of tongue (2 patients). Left side location was noted in 65 patients and right side in 33 patients. Histopathologically, there were 66 well differentiated, 6 moderately differentiated, and 11 less well differentiated tumors. Differentiation was not documented in 15 patients.
All 98 patients received partial glossectomy, with 14 patients receiving partial glossectomy with elective neck dissection and 84 patients receiving partial glossectomy only. The partial glossectomy only group (PG group) consisted of 84 patients (47 males, 37 females). Of these, 61 patients had a T1 primary tumor, while 23 patients had a T2 primary tumor. The partial glossectomy with elective neck dissection group (END group) consisted of 14 patients (9 males, 5 females), 9 of whom had T1 primary tumor, while 5 patients had T2 primary tumor. The patients are described in Table 1.
Of the total cases, 17 experienced occult cervical metastasis, including pathologically positive metastasis in 4 cases in the elective neck dissection group and neck metastasis in 13 cases in the primary resection without elective neck dissection group. The total prevalence of occult metastasis was 17.3%. The incidence of T1 and T2 occult metastasis were 17.1% and 17.9%, respectively.
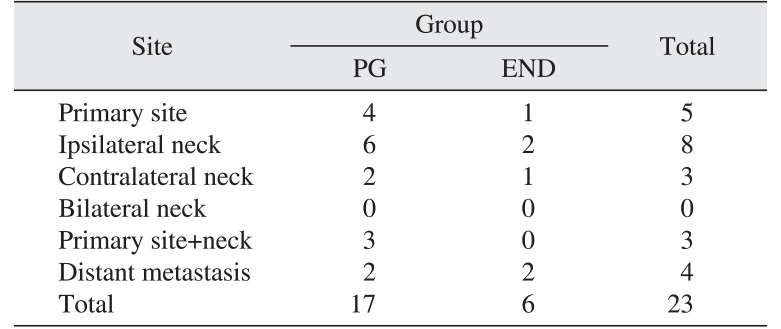
In the PG group, a total of 15 patients experienced locoregional recurrence, located as follows: primary site only (4 cases), primary site+neck (3 cases), and neck only (8 cases). All patients had surgical salvage. Distant metastasis occurred in 2 patients, both of whom had also experienced previous locoregional recurrence. In the END group, a total of 4 patients demonstrated locoregional recurrence, located as follows: primary site only (1 case) and neck only (3 cases). All patients had surgical salvage. Distant metastasis occurred in 2 patients, and 1 patient had previously been diagnosed with locoregional recurrence.(Table 2)
The 5-year OS rate for all patients was 90.8%, and the DFS rate was 67.1%. The 5-year DFS rates of T1 and T2 were 71.1% and 54.3%, respectively.
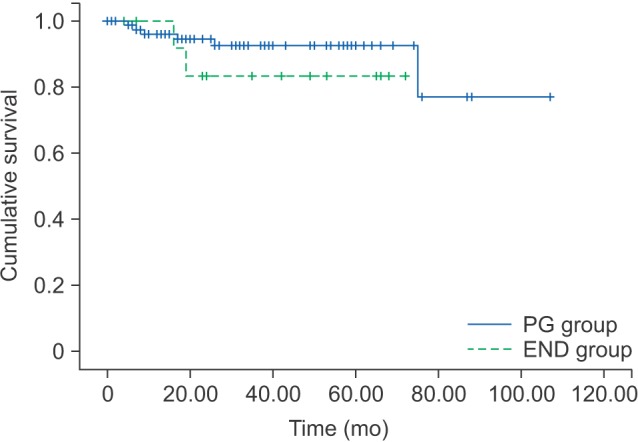
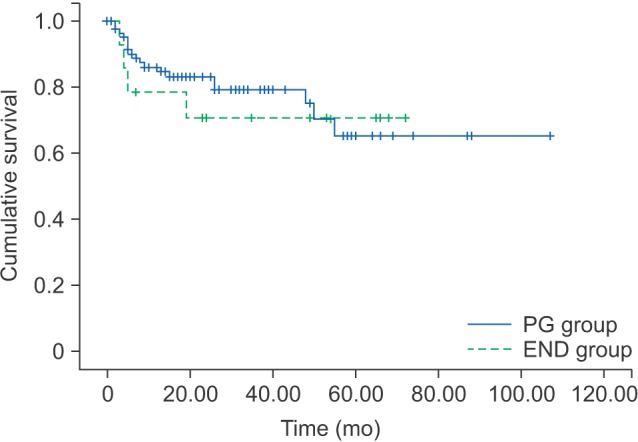
The 5-year OS and 5-year DFS rates for the PG group were 92.4% and 65.3%, respectively. The 5-year OS and 5-year DFS rates for the END group were 83.3% and 70.7%, respectively.(Table 3) By log-rank test, the OS (P=0.325) and DFS (P=0.728) were not significantly different between the PG and END groups.(Fig. 1, 2)
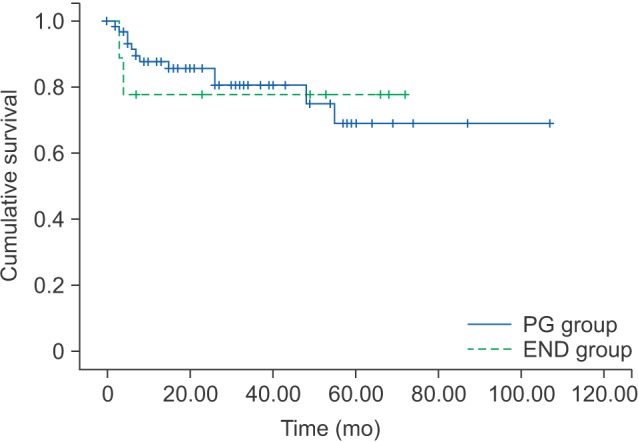
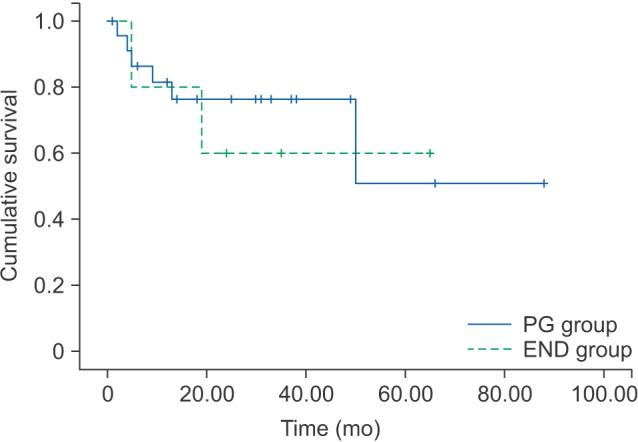
The 5-year OS and DFS rates of the PG and END groups in T1 and T2 patients are shown in Tables 4 and 5, respectively. By log-rank test, the DFS was not significant statistically different between the PG and END groups in T1 (P=0.961) or T2 (P=0.765).(Fig. 3, 4)
Univariate analysis demonstrated that patients with recurrence had significantly shorter OS and DFS. Age, gender, tumor site, histological grade, elective neck dissection, and T staging were not prognostic factors. By multivariate analysis, recurrence and gender were independent factors affecting DFS. Elective neck dissection showed no prognostic effect in OS, and recurrence was the only independent factor affecting OS.(Table 6)
IV. Discussion
We retrospectively analyzed our results of the efficacy of elective neck dissection in stage I and II tongue SCCa with clinically N0 grading in the neck.
The presence of cervical lymph node metastasis is a major determinant of prognosis and treatment in tongue SCCa. As mentioned before, the occult metastasis rate ranged from 7%-33% in T1 and 28%-53% in T2 in the clinically N0 tongue SCCa patients. In this study, the risk of occult neck metastasis also increased according to T stage. The overall rate of occult metastasis was 17.3% (17.1% in T1 and 17.8% in T2), which was comparable with the occult metastasis in other studies.
Our data demonstrated that the 5-year OS rate in the PG and END groups was 92.4% and 83.3%, respectively, and the 5-year DFS rate in the PG and END groups was 65.3% and 70.7%. There was no significant difference between the two groups. The results from our study show that END cannot significantly improve survival for patients with stage I or II tongue SCCa compared with PG. Other studies also found it difficult to show an improvement of survival after elective neck dissection. Keski-Säntti et al.15 reviewed 80 patients with T1 or T2 with clinically N0 neck nodes in tongue SCCa and reported that elective neck dissection did not increase DFS or OS. Liu et al.1 demonstrated no statistical differences in DFS or OS between END and PG groups. In contrast, Kligerman et al.21 reported that elective neck dissection increased the 3-year survival rate from 49% to 72%.
In T1 patients, the 5-year DFS rate for the PG and END groups was 68.8% and 77.8%, respectively. In T2 patients, this 5-year DFS rate was 51.0% and 60.0%, respectively.
As shown in this study, gender and recurrence were independent factors affecting DFS, while only recurrence was an independent factor affecting OS. Elective neck dissection was not an independent predictive factor of OS or DFS by univariate or multivariate analysis. Therefore, elective neck dissection could not significantly improve the OS or DFS in early (stage I or II) tongue SCCa. Age, histological grade, tumor site, and stage also showed no prognostic effect in stage I or stage II tongue SCCa.
V. Conclusion
In conclusion, this study showed that elective neck dissection did not have a significant benefit in terms of survival in the management of clinically N0 neck of early stage tongue SCCa. Routine recommendation of elective neck dissection of clinically N0 neck is not advisable. We conclude that careful selection of elective neck dissection can be of help to the patient. In the future, a prospective randomized study will be useful to further evaluate the benefit of neck management in the treatment of the early stage (stage I or II) tongue SCCa.




 XML Download
XML Download