

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Caries and periodontal disease are the main reasons for tooth loss, although other factors are also contributory. Tooth loss can result from change in food choices and nutrition, leading to medical problems affecting one's general health. Tooth loss can also have a negative impact on emotions and oral health with relation to quality of life123. In the last two decades, dental implants (DI) have been used as a common treatment modality due to their high success rate. Considering the high success rate (95%), approximately 450,000 osseointegrated DI are being placed every year with minimal complications4.
The mainstay for the placement of DI is the availability of an adequate amount of alveolar bone. Following tooth extraction, wound healing of the socket is subjected to modeling and remodeling processes, leading to dimensional alterations of the residual ridge5. The dimensional changes can lead to reduced height and width of the bone, thus limiting the insertion of a DI of desired length and diameter67. Furthermore, the complications involved with any other surgical procedure can also be seen with DI surgery89. Damage involving nerves, the inferior alveolar artery, and encroachment into the maxillary sinus can cause numbness and tingling sensations, hemorrhage, and development of oroantral communication, respectively8. These factors mandate a proper radiographic assessment prior to DI placement. The radiographic technique must be accurate enough to provide details of anatomic structures and the morphology of the implant site and its bone density together with information on abnormalities and disease10. The American Academy of Oral and Maxillofacial Radiology (AAOMR) has recommended computed tomography (CT) for implant site assessment, including precise measurement of distances in three dimensions 1112.
The introduction of the CBCT technique is the biggest milestone in the field of dentistry, allowing for three-dimensional diagnosis. The literature has shown many applications of CBCT in DI treatment planning, particularly with regards to linear measurements, three-dimensional evaluation of alveolar ridge topography, visualization of vital anatomical structures, and construction of surgical guides1314. The advantages of CBCT over conventional imaging include the absence of superimposition and image magnification, shorter scanning time, and a lower radiation dose than multi-slice CT13. The availability of the CBCT has increased in dental offices because of these advantages1314.
Our study is the first of its kind in this region and is aimed at localization of the mandibular canal (MC) and measurement of the height and width of the available alveolar bone at the proposed implant site in the posterior segment of the mandible using CBCT in patients with a single missing tooth.
II. Materials and Methods
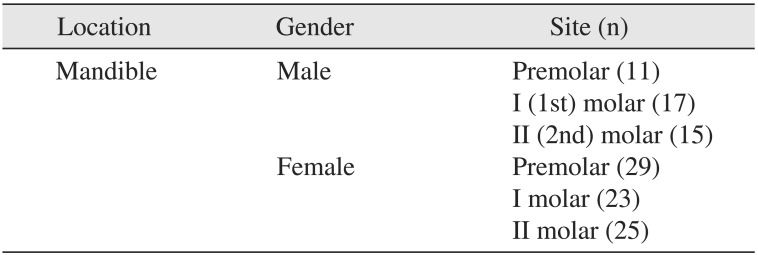
This research was performed in accordance with the ethical principles of the Riyadh Colleges of Dentistry and Pharmacy Research Center and the College of Dentistry Research Center, King Saud University. The study was carried out during the period from March 2014 to December 2015. A power analysis was performed to determine the sample size, with a non-directional alpha risk of 0.05 and a power of 83%. This is a retrospective study, in which a total of 91 CBCT scans, with single missing premolar, I (1st) molar, or II (2nd) molar, were collected from multiple dental centers in Riyadh City. The study was composed of 40 males and 51 females, aged between 14-56 years. A total of 120 mandibular sites with 40 sites of one of the three missing types of teeth were selected to measure the height and width at the premolar, I molar, and II molar areas.(Table 1) CBCT scans that revealed severe periodontal disease, total loss of posterior teeth and signs of fracture, oral surgical procedures, or pathological lesions were excluded from the study.
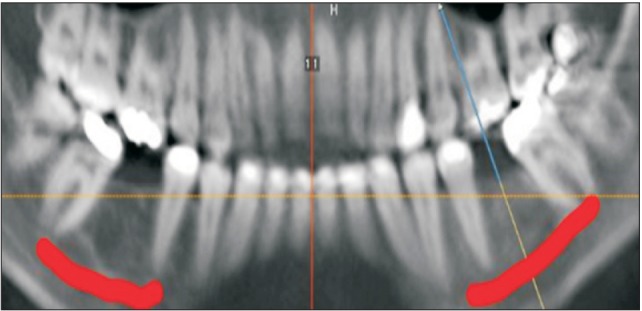
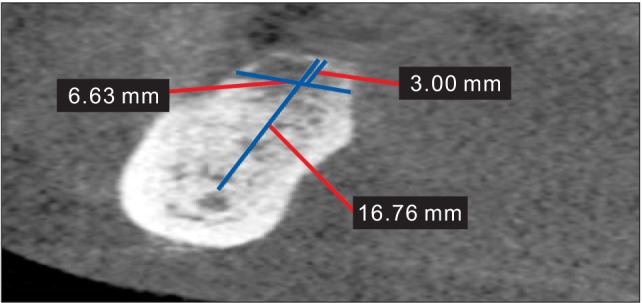
All scans were analyzed using OnDemand3D software (version 1.0; CyberMed Inc., Seoul, Korea) by two investigators (oral radiologist and periodontist). First, for each CBCT scan, the axial cut (Fig. 1) was adjusted according to the edentulous region. An arch curve line was then drawn through the adjacent teeth roots to produce a panoramic image (Fig. 2), and the MC was traced. Afterward, at the proposed implant placement site, a cross-sectional view was selected to measure the vertical height (from the superior margin of the MC to the crest of the alveolar ridge) and bucco-lingual width (3 mm below the crest of the alveolar ridge). (Fig. 3) For reliability, 10 cases were selected randomly and measured twice at different times by each examiner independently in order to determine inter- and intra-examiner reliability. There was good (0.83) inter-examiner agreement and excellent (0.97) intra-examiner agreement between the two examiners. Data was collected, tabulated, and statistically analyzed using independent t-test, with a P-value ≤0.05 considered statistically significant (IBM SPSS Statistics 23.0; IBM Co., Armonk, NY, USA).
III. Results
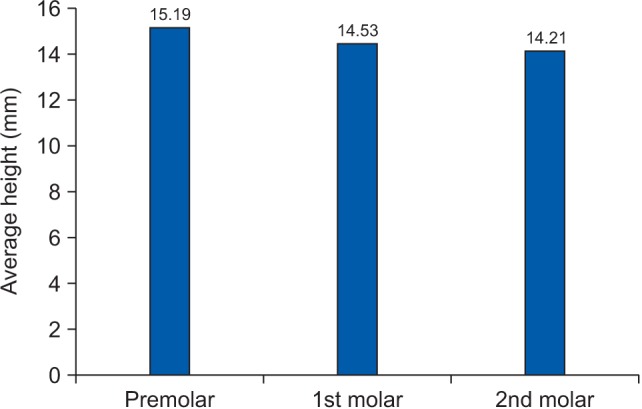
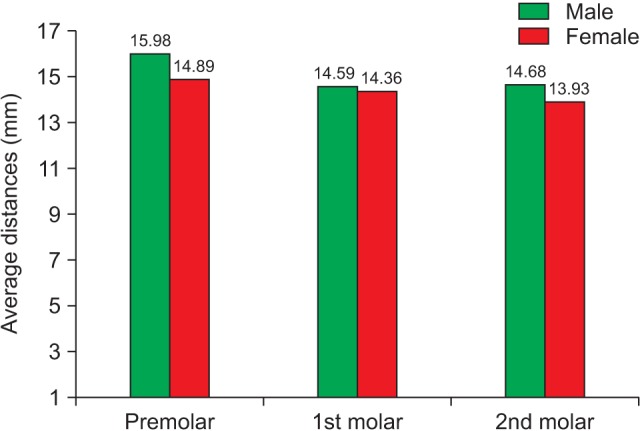
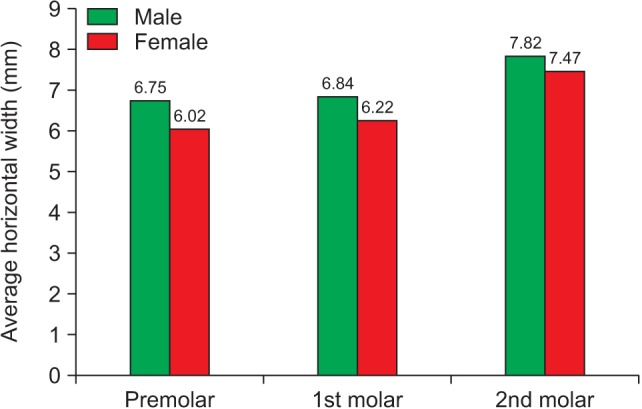
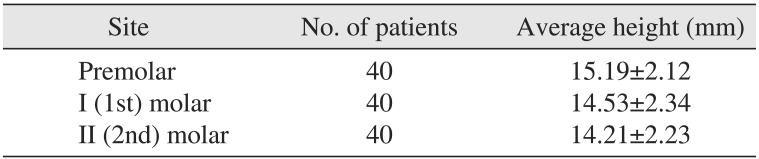
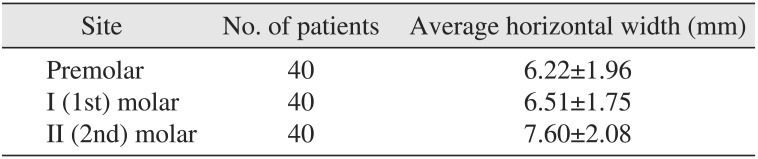
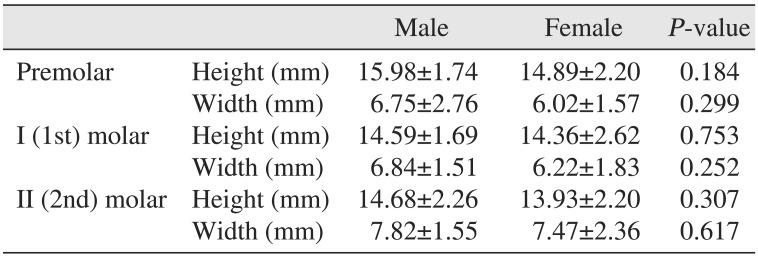
The average height from the alveolar crest to the superior position of the MC at the premolar, I molar, and II molar areas was 15.19±2.12 mm, 14.53±2.34 mm, and 14.21±2.23 mm, respectively, as shown in Table 2 and Fig. 4. The average widths measured 3 mm below the crest of the alveolar ridge in the mandible at premolar, I molar, and II molar areas were 6.22±1.96 mm, 6.51±1.75 mm, and 7.60±2.08 mm, respectively, as shown in Fig. 5 and Table 3. The gender differences between the height and width mean values are illustrated in Fig. 6 and 7. There was no statistically significant difference between males and females regarding vertical or horizontal measurements of the alveolar ridges, as shown in Table 4.
IV. Discussion
Complications are increasing with the increased utilization of DI for missing teeth. It is crucial to identify and localize vital structures (maxillary sinus and MC) during DI treatment in order to provide quality dental care 15161718. CBCT images are ideal for linear measurements in the posterior regions of the mandible and maxilla and provide satisfactory localization of the anatomical vital structures19. This study was designed to assess the MC location and availability of remaining bone for the placement of DI using CBCT. To the best of our knowledge, this is the first study to three-dimensionally evaluate the mandibular posterior segment with a single missing tooth on CBCT scans in a large cohort of individuals.
Considering the cross-sectional nature of our study, some of the variables (traumatic episodes during extraction, presence of endodontic/periodontal lesions before extraction, type of prosthetic rehabilitation after tooth removal, and lack of information on the healing time following tooth extraction) that can influence the dimensions of remaining bone were not considered.
The data from the available literature related to the height and width of the alveolar bone and localization of the MC are compiled in Tables 5 and 6. In 2010, Kilic et al.20 performed a study on 49 hemi mandible specimens (cadavers) and found the mean distance from the alveolar crest to the superior position of the MC to be 12.63 mm for the edentulous area of premolars, 12.50 mm for the edentulous area of I molars, and 13.07 mm for the edentulous area of II molars. The current study showed that the mean distance of the corresponding area was 15.19 mm for the edentulous areas of premolars, 14.53 mm for the edentulous areas of I molars, and 14.21 mm for the edentulous areas of II molars. The slight differences in results might be because Kilic et al.20 used totally edentulous areas in their study, while the present study measured single-tooth edentulous sites. The dimensions of the alveolar ridge can be influenced by the presence or absence of teeth adjacent to the edentulous site based on the assumption that the presence of adjacent teeth can, to some extent, limit the remodeling of the alveolar crest following tooth extraction. Furthermore, it can be speculated that the extraction of multiple adjacent teeth might result in greater bone crest resorption due to the lack of vascular support to the interdental alveolar process from the periodontal vascular supply of the adjacent teeth. However, not enough data is available on the influence of multiple, adjacent extraction sites vs. single, isolated tooth extractions on the measurements of the edentulous ridge21.
de Oliveira Júnior et al.22 in 2011, reported that the average distance of the alveolar crest to the superior position of the MC at the premolar, first molar, and second molar areas was 16.10±2.52 mm, 16.40±2.65 mm, and 16.70±3.41 mm, respectively. In the present study, the average distance of the alveolar crest to the superior position of the MC at premolar, I molar, and II molar areas was 15.19±2.12 mm, 14.53±2.34 mm, and 14.21±2.23 mm, respectively. Their results were higher than our current results, possibly due to their mixed (dentulous and edentulous) samples, whereas the present study measured single-tooth edentulous sites only. This could be also supported by the recorded difference between the Levine et al.23 findings in 2007, where the distance from the alveolar crest to the superior aspect of the inferior alveolar canal was 17.4±3.0 mm in the area of the I molars, while a smaller value of 14.53±2.34 mm was found in the present study because Levine et al.23 measured the heights of dentulous patients compared to this study where only edentulous sites were measured.
In 2010, Watanabe et al.24 studied CT data of both dentulous and edentulous cases of 79 Japanese patients. The mean values of the measured distances from the superior border of the MC up to the alveolar crests in the premolar, I molar, and II molar regions (15.3-17.4 mm) were higher than the values in this study (14.2-15.2 mm), which might be due to their sample.
In 2004, Frei et al.25 studied edentulous mandibular I molar sites for 35 patients and found that the average height from the MC to the alveolar crest in linear tomography was 14.87±3.3 mm. This finding is in agreement with our study, which showed that the average measured bone height from the MC to the alveolar crest in CBCT for edentulous mandibular I molar sites was 14.53±2.34 mm.
In 2012, Braut et al.26 studied 56 CBCTs and measured the horizontal bucco-lingual width of dentulous mandibular alveolar ridges and the mean width for premolar, I molar, and II molar regions as 7.6 mm, 10.2 mm, and 9.8 mm, respectively. However, mean widths in the current study were 6.22 mm, 6.51 mm, and 7.60 mm, respectively. The lower values in the current study could be attributed to the fully dentulous subjects used in the previous study.
The studies from Shahin et al.18, de Oliveira Júnior et al.22, Levine et al.23, and Watanabe et al.24 regarding the position of the MC found no significant difference between males and females in the location of the MC. These results are in accordance with the present study, which showed no significant difference between males and females regarding distances from the alveolar crest to the superior position of the MC.
In 2012, Braut et al.26 studied 56 CBCTs and found that sex was a statistically significant parameter for bone height, with male patients exhibiting higher values than females. This could be due to the fully mandibular dentulous subjects used in the study.
V. Conclusion
Our study aimed at localizing the MC and estimating the remaining alveolar bone (height and width) in patients with a single missing tooth in the posterior segment of the mandible. The measurements were averaged separately for each of the single missing teeth (premolar, I molar, and II molar), which gave more accurate information for DI placement. Further research should compare the findings with fully dentulous and edentulous patients as well as determine the influence of prosthetics with a note on the time length of edentulousness.




 XML Download
XML Download