

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
The initial management of the neck in early oral squamous cell carcinoma (OSCC) with clinically negative neck nodes (clinical T stage [cT] 1 or 2 and clinical N stage [cN] 0) remains a controversy. Before the 1990s, the traditional policy for management of the clinically negative neck in early OSCC was generally a ‘wait-and-see’ or observation (OBS) policy, unless the neck was being opened for other reasons such as better access to the primary tumor, reconstruction requirements, or delaying neck dissection until cervical metastases was clinically evident.
The incidence of occult regional lymph node metastasis of OSCC varies from 6% to 46%, according to previous reports1. Once regional metastases have occurred, the 5-year survival rate for patients with oral cancer decreases by one-half relative to that of patients with early-stage disease23. In view of the high incidence of nodal recurrence of the observed neck, prophylactic neck dissection has been advocated as a routine management protocol of N0 neck4.
The results of the few prospective randomized studies and a retrospective study on the benefit of prophylactic neck treatment have been inconclusive. The studies failed to find statistically significant differences in prognoses between the groups of patients under OBS without initial neck dissection and those groups initially managed with neck dissection567.
The aim of this study was to retrospectively review and compare the outcomes between patients under OBS and patients who underwent elective neck dissection (END) at initial surgery and to identify factors that affect locoregional control and survival.
II. Materials and Methods
This retrospective study included 215 OSCC patients who underwent surgical treatment at Department of Oral and Maxillofacial Surgery, Yonsei University Dental Hospital (Seoul, Korea) from 1990 to 2012, based on a screening of medical records. This study was approved by the regional Ethical Review Board of Yonsei University Dental Hospital Institutional Review Board (IRB No. 2-2014-0032). Patients with recurred tumor, second primary tumor, metastatic tumor, and patients who underwent salvage surgery were excluded. Patients who had clinically T3 or T4 tumor were also excluded. Patients with positive neck nodes on physical exam or imaging studies, including computed tomography (CT), magnetic resonance imaging, positron emission tomography (PET), PET-CT, and ultrasonography, were excluded. After the selection process, 79 patients were suitable for analysis. Among them, 52 patients underwent END and 27 patients did not receive neck dissection and underwent OBS only.
Following the policy of most institutions, OBS was applied when there was no evidence of neck node metastasis, and END was applied to patients with suspicion of neck node metastasis despite negative results.
In the OBS group, occult cervical metastasis was defined as a neck recurrence during follow-up, without failure at the primary site89. Cervical metastases in patients with recurrent primary tumor were not considered occult metastases because the nodal spread may have occurred after the initial treatment89. In the END group, occult disease was defined as the presence of microscopic disease on the histopathologic examination of neck dissection specimens89.
Survival curves were plotted using the Kaplan-Meier method and compared using the log-rank test. Chi-squared test or Fisher exact test was used for categorical data analysis. Univariable analyses were performed to find factors affecting recurrence. For multivariable analyses to find independently related factors of recurrence and survival, the Cox proportional hazard model was used. Differences were considered significant for P-value <0.05. All statistical analyses were performed with PASW Statistics software version 18.0 (IBM Co., Armonk, NY, USA).
III. Results
1. Characteristics of the study population
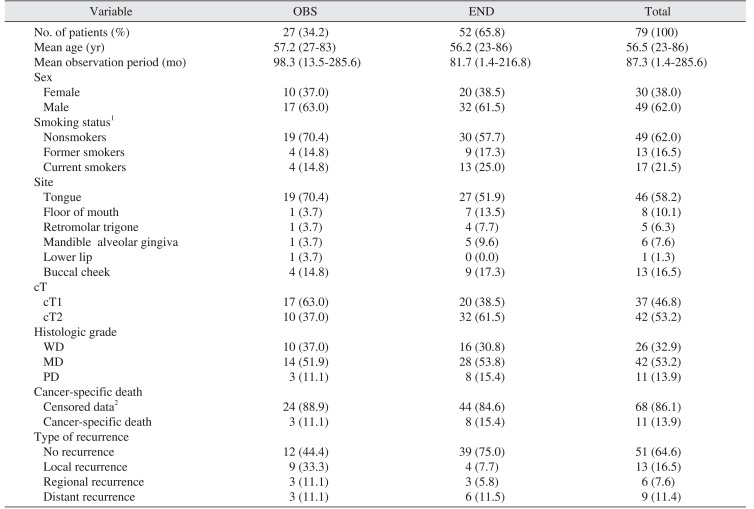
The patients were divided into two groups: OBS (n=27, 34.2%) and END (n=52, 65.8%). The median age of the entire group was 59 years. The OBS period varied from 1.4 months to 285.6 months with a mean of 87.3 months. Regarding the site of primary lesion, 46 (58.2%) were from tongue, 13 (16.5%) from buccal cheek, 8 (10.1%) from floor of mouth, 6 (7.6%) from mandibular alveolar gingiva, 5 (6.3%) from retromolar trigone, and 1 (1.3%) was from maxillary alveolar gingiva. The stages were cT1 and cT2 in 17 patients (63.0%) and 10 patients (37.0%) in the OBS group, respectively, and 20 patients (38.5%) and 32 patients (61.5%) in the END group. In total, there were 37 patients (46.8%) with cT1 stage and 42 patients (53.2%) with cT2 stage. The characteristics of the study population are shown in Table 1.
2. Characteristics of nodal metastasis
Characteristics of nodal metastasis were investigated in the END group. Forty-two cases (42/52, 80.8%) were pathologically confirmed as negative for neck node metastasis (pN0). Among the remaining 10 cases (10/52, 19.2%), 8 (15.4%) were pN1, and 2 (3.8%) were pN2. Forty-one patients (78.8%) underwent ipsilateral selective neck dissection (SND). Six patients (11.5%) underwent bilateral SND, and 5 patients (9.6%) underwent modified radical neck dissection.
3. Survival analyses
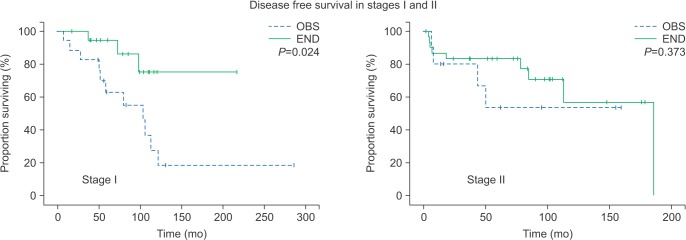
The END group showed a statistically significant benefit in disease-free survival (P=0.027; Fig. 1), especially in stage I patients (P=0.024).(Fig. 2) However, there was no statistically significant difference in regional recurrence-free survival or cancer-specific survival between OBS and END groups. (Fig. 3, 4)
4. Occult metastasis
Occult cervical nodal metastases were found in 13 cases (13/79, 16.5%), including neck recurrence in 3 cases of the OBS group (3/27, 11.1%) and pathologically positive metastases in 10 cases of the END group (10/52, 19.2%). In univariable analysis, occult metastasis was related to higher odds of cancer-specific death (odds ratio [OR]=6.25, P<0.01).
5. Factors of overall recurrence
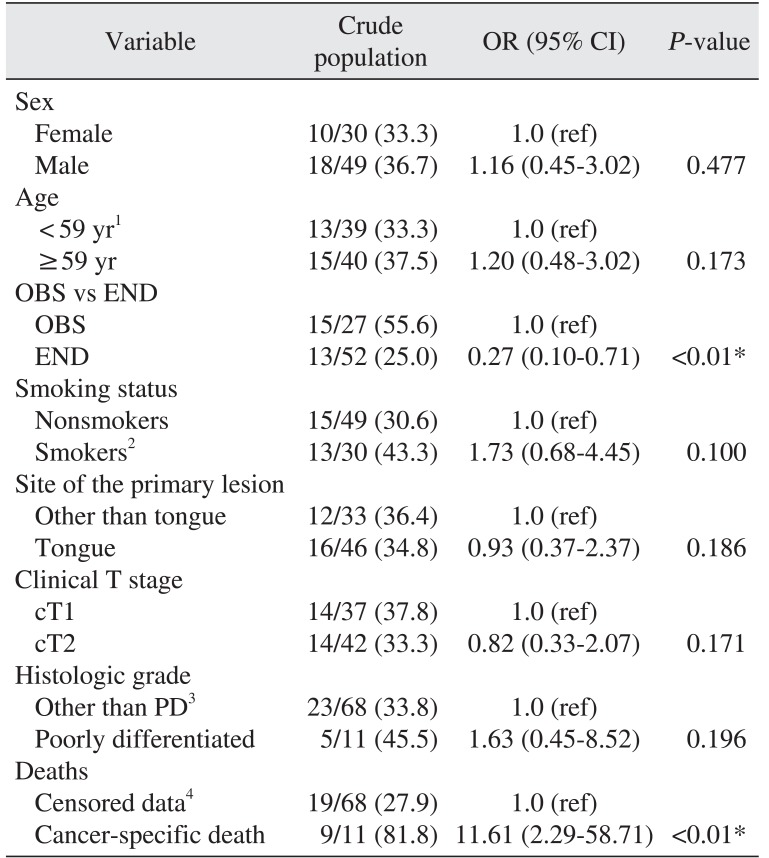
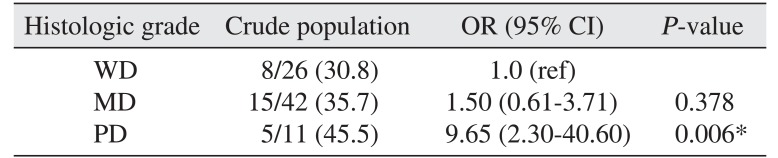
To determine the factors related to overall recurrence, we performed univariable and multivariable analyses. In univariable analyses, the END group was correlated with lower overall recurrence (OR=0.27, P=0.006).(Table 2) Cancer-specific death was related to higher odds of overall recurrence (OR=11.61, P<0.01).(Table 2) In multivariable analysis, poor histologic grade was independently related to overall recurrence (OR=9.65, P<0.01).(Table 3)
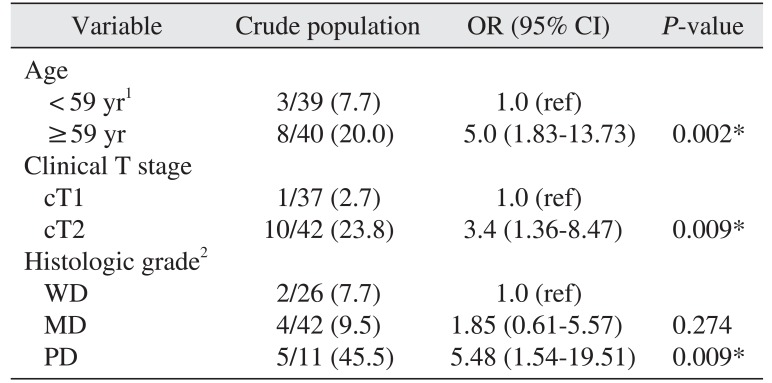
6. Factors of cancer-specific death
In a multivariable analysis, advanced age (OR=6.3, P=0.022), higher clinical T stage (OR=15.2, P=0.01), and poorly differentiated histologic grade (OR=6.6, P=0.025) were independently related to cancer-specific death.(Table 4)
IV. Discussion
A therapeutic neck dissection is obviously necessary when clinically invaded nodes are present10. The presence of regional neck metastases is widely accepted as a major determinant of prognosis in patients with OSCC1112. If the probability of neck metastases is high, a neck dissection will decrease the risk of regional recurrence. However, if the probability of neck metastases is low, neck dissection constitutes overtreatment, where the morbidity of the neck procedure only decreases quality of life while increasing functional deficits. While the problem could be solved if it were possible to predict the risk of neck metastases, such prediction has been difficult to introduce and apply in clinical practice. Finally, there is little published guidance about management of the N0 neck in OSCC13.
Patients with cT1N0 and cT2N0 OSCC have been reported to have occult metastases in 13% to 33% and 37% to 53% of cases, respectively, at the time of diagnosis14. In this study, the overall occult cervical nodal metastatic rate was 16.5% (13/79). The rates for cT1N0 and cT2N0 in this study were 8.1% (3/37) and 23.8% (10/42), respectively. Though the occult metastasis rate is relatively low in our study, the tendency toward comparably higher incidence of occult metastasis in T2 compared to T1, as well as ipsilateral neck being the common site of recurrence, seem congruent with results from previous studies9.
An interesting result of our study is that the END group was related to lower recurrence, but did not seem related to better survival. Of course, we should carefully interpret these results since this study was a retrospective analysis and not a double-blind prospective randomized control trial, so a selection bias (i.e., predilection of END for advanced T stages) may have influenced the results. Most studies have focused on the rate of occult metastasis and related factors to demonstrate the necessity of END. Our results tentatively suggest that END may lower the rate of recurrence, but not necessarily improve survival, and that the characteristics of the tumor itself, such as clinical T stage and poor histologic grade, may be important for survival. These results may be helpful when determining the necessity of END for early stage OSCC.
Previous studies have suggested other factors that influence final outcome and survival of cancer treatment. Eicher et al.15 recommended END for patients with moderately or poorly differentiated SCC, radiological or histological signs of bony invasion, and tumors in the mandibular symphyseal region16. Ogura et al.17 examined mandibular bony invasion using dental CT and found it unfavorable as a prognostic indicator of 5-year survival.
Feng et al.11 reported that the follow-up compliance of patient populations was the vital factor in adopting the OBS strategy for the cN0 neck. They stated that early detection of regional recurrence led to a 100% cervical salvage rate irrespective of T stage, the salvage rate otherwise dropping as remarkably low as <30.0%11. They concluded that END should be recommended as first-line management for all intermediate and advanced stage patients, with the exception of patients with stage T1 tumors, who have a low risk of nodal metastasis and for whom OBS may be an acceptable alternative to END if the patients strictly comply with a cancer surveillance protocol11.
V. Conclusion
For better survival of early OSCC patients without clinically evident neck node metastasis, characteristics of the tumor itself, such as advanced T stage and poor histologic grade, may be equally or more important than the treatment modality of the neck. The follow-up compliance of the patients must be guaranteed to adopt the OBS strategy for the cN0 neck.



 XML Download
XML Download