

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Difficulty in securing an airway is often experienced in the management of complex maxillofacial trauma. Modern techniques for surgical treatment of midfacial and panfacial fractures in maxillofacial trauma pose special problems for airway management. According to a recent review, submental intubation is a useful alternative technique for airway management in patients with panfacial fractures1, although it can have side effects such as tracheal stenosis, subcutaneous emphysema, bleeding, laryngeal nerve injuries, and tracheal esophageal fistula23.
Submental intubation as an alternative for tracheotomy was first introduced and described by Hernández Altemir4 in 1986, and it has been shown to be an efficient airway management technique in patients with several maxillofacial injuries25. The technique is performed as endotracheal tube proximal end deflection from under the chin, with a small incision after typical oral intubation35. This method is useful for patients who require long-term mechanical ventilation, such as those with multiple injuries, severe neurological trauma, severe thoracic trauma, or those undergoing a repeat contradicted surgery67. In comparison to tracheotomy, submental intubation has fewer side effects; many studies have described it as a quick, simple, and safe technique for airway management7. Therefore, authors aimed to report a case of submental intubation during maxillofacial surgery with a contraindication of fracture in the lower jaw.
II. Case Report
The patient was a 23-year-old male weighing 72 kg who was admitted to the Accident and Emergency Department of Imam Khomeini Hospital (Sari, Iran) after a motorcycle accident, which had resulted in some fractures of his lower jaw. He was intubated and connected to a ventilator for 10 days. At this time, the patient's consciousness level improved, the ventilator and endotracheal tube were disconnected, and he transferred to another hospital in order to undergo maxillofacial surgery for treatment of lower jaw fractures. The patient was scheduled for surgical correction of multiple facial fractures on the same day.
1. Procedure
The results of the patient's laboratory test and vital signs were normal; hemoglobin, 13 g/dL; PH, 7/35℃; SpO2, 98%; blood pressure, 130/70 mmHg; heart rate, 85/min. The patient fasted for 8 hours prior to the operation and was pretreated with 2 mL fentanyl, 2 mg midazolam, 20 mg lidocaine, 200 mg propofol, and 100 mg succinyl-CoA before induction. The technique used for submental intubation was an adaptation of the general method published by Hernández Altemir4.
Considering the probability of a challenging intubation, the patient was intubated orally with a reinforced (spiral-embedded) tracheal tube with an internal diameter of 7.5 mm. The orotracheal intubation was then converted to a submental endotracheal intubation using the following procedure.
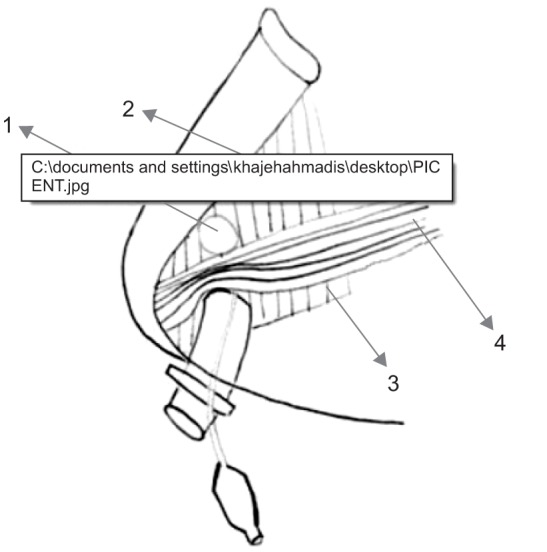
After sterile painting and draping of the chin and mouth, lignocaine 2% with 1:80,000 adrenaline was infiltrated into the incision site. A midline incision 1.5 cm in length was made anterior to the inferior border of the mandible at the chin level. A curved hemostat was passed from the submental incision through the subcutaneous layer, platysma, mylohyoid muscle, submucosal layer, and mucosa. After entering the oral cavity at the junction of the attached lingual alveolar mucosa and the free mucosa of the floor of the mouth, an incision 1.5 cm in length was made parallel to the gingival margin. Then, based on bilateral symmetric lungs sounds, the patient was connected to a ventilator through a manual ambo bag. A 1.5 cm incision was made in the right submental region parallel and medial to the inferior border of the mandible. The endotracheal tube was briefly disconnected from the breathing circuit, and the tube connector was removed from the tube. A pilot balloon connected to the endotracheal tube was gently removed through the incision.(Fig. 1)
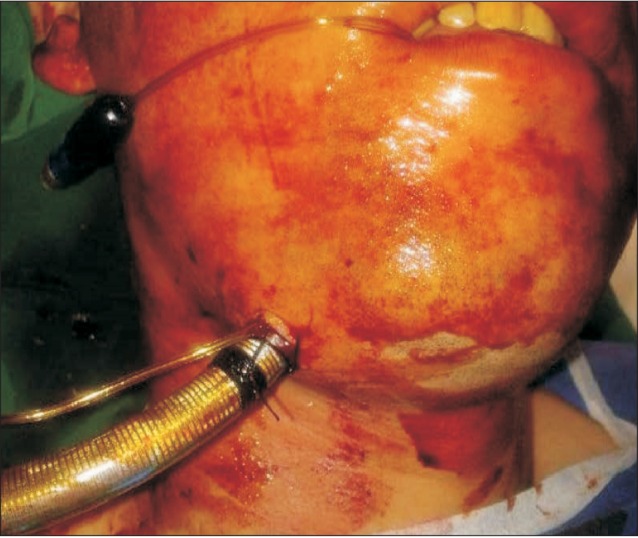
Following tube removal, audible lung sounds, and assurance of the appropriate location of the submental tube, a number 18 tube was fixed under the patient's chin, and the patient was connected to the ventilator.(Fig. 2)
At the end of surgery, submental intubation was converted to oral intubation. The surgery lasted two hours and involved no particular problems. The patient's blood pressure ranged between 100 and 130 mmHg during surgery. In addition, the postoperative period was uneventful. There was no episode of arterial desaturation while converting oral intubation to submental intubation and vice-versa.
III. Discussion
Submental intubation was introduced as a substitute for oral or nasal intubation, especially in extensive maxillofacial injuries. It has been used for years, and no serious side effects have been reported36. Many studies have described submental intubation as a simple, quick, and safe method for airway management1235678. This method does not produce the side effects associated with other methods such as nasal bleeding, meningitis, skull base fracture, tracheal stenosis, neck vessel injuries, or thyroid or subcutaneous emphysema567. The Escher of submental intubation is not as significant as that of tracheotomy and is tolerable by patients3.
Some possible side effects of submental intubation include accidental ejection of the tube, sudden movement of the tube into the main bronchus, bleeding or hemorrhage, infection, and salivary gland and meatus trauma7. Although these effects have been rarely reported. Meyer et al.8 reported mouth floor abscess in 8% of their patients and hypertrophic Escher in 4%. Schütz and Hamed9 performed a comparative study between submental intubation and tracheostomy and concluded that submental intubation is associated with low morbidity and can replace tracheostomy in selected cases of maxillofacial trauma.
However, Caubi et al.3 observed airway pressure increase in a patient due to the excessive angle of the endotracheal tube in the oropharynx. MacInnis and Baig10 also reported the long ventilation in submental intubation leads to problem. They found that submental intubation might result in a delay in airway establishment.
Our patient tolerated this method successfully. We established an assured airway and sufficient space for the surgeon to handle and fix the facial fractures. This experience is in line with a comprehensive literature review of 812 patients by Jundt et al.11, which reported a 100% success rate of submental intubation and only minor complications. After surgery, the present patient was transferred to the intensive care unit, where he regained complete consciousness. The endotracheal tube was then removed, and the patient was discharged 2 days later. No complication was noted, and the submental scar was almost invisible after 2 months.
 XML Download
XML Download