

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Aortic aneurysm is a serious condition characterized by the tearing of the inner layer of the aorta. It can lead to sudden death caused by cardiac failure and occasionally, aortic rupture12. In addition, hypertension can increase the stress on the weakened aortic wall, increasing its susceptibility to tearing. Aortic aneurysms are divided into Stanford type A and Stanford type B dissections. While type B dissections generally are initially treated medically, with surgery reserved for complications, type A aortic aneurysms, which involve a tear in the aorta ascendens, generally require emergency or quasiemergency surgical treatment2.
Dexmedetomidine (DEX) is an anti-anxiety, sedative, and analgesic medication that can stabilize circulatory dynamics3 and minimize blood pressure fluctuations.
We report a case of a 45-year-old morbidly obese man with an aortic aneurysm (Stanford types A and B), in whom invasive oral treatment, namely tooth extraction and cyst enucleation, for the removal of intraoral infectious sources, was successfully performed under local anesthesia with DEX sedation before elective cardiac surgery.
II. Case Report
A 45-year-old morbidly obese man was transported by ambulance to the Emergency Medical Care Center at Fukuoka University Hospital (Fukuoka, Japan) with suspected acute heart failure after developing a sudden difficulty in breathing with pink frothy sputum. According to his wife, the patient had no significant medical history other than hypertension. Detailed examination revealed an aortic aneurysm (Stanford types A and B), aortic regurgitation, aortic valve ring ectasia, ascending thoracic aorta aneurysm, hypertension, paroxysmal tachycardia, atrial fibrillation, primary lung cancer in the left lower lobe, and morbid obesity (weight, 124 kg; height, 170 cm; body mass index [BMI], 42.9 kg/m2). The aortic aneurysm required emergency surgery. However, because of the patient's morbid obesity, elective vascular graft replacement of the thoracic ascending aorta, aortic valve replacement, pulmonary vein isolation surgery, and segmental left lower lobe resection were planned after gradual weight reduction with dietary therapy. On hospital day 16, the patient underwent a preoperative detailed intraoral examination in our department. At the patient's first visit to our department, his weight was 109 kg (BMI, 37.7 kg/m2). Intraoral examination revealed six teeth with periapical lesions and two pigeon eggsized radicular cysts that could become potential sources of infection after surgery.(Fig. 1)
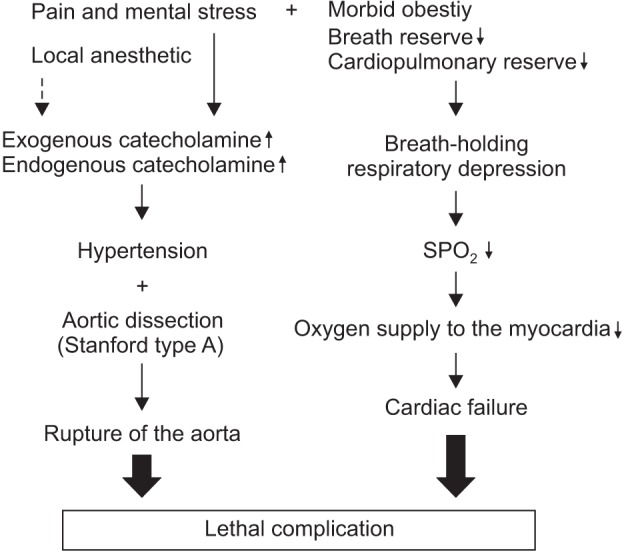
The patient was at increased risk of developing severe complications of aortic aneurysm such as cardiac failure and rupture of the aorta through a sudden increase in blood pressure 12.(Fig. 2) The use of intravenous sedation was deemed appropriate to avoid sudden changes in blood pressure and to stabilize the patient's hemodynamics. The patient's respiratory depression due to morbid obesity also required attention. Accordingly, we planned to use DEX4, which is reported to cause mild respiratory depression, for sedation. The surgery and sedation procedure were explained to the patient, and informed consent was obtained. The surgery involved three oral surgeons, one board-certified dental anesthesiologist, and one nurse. The patient was required to fast for six hours before the procedure. We adopted Fowler's position during the surgery, and vital signs (peripheral capillary oxygen saturation, heart rate, blood pressure, and electrocardiogram) were continuously monitored. Oxygen was administered at 3 L/min through a nasal cannula. An initial loading dose of DEX was administered at 4.4 µg/kg/hr for 10 minutes, followed by continuous infusion at 0.075 to 0.3 µg/kg/hr. The procedure took 1 hour 27 minutes to complete, with stable hemodynamics throughout and no marked changes, even during local anesthesia with 2% lidocaine and 1:80,000 epinephrine.(Fig. 3) Surgery was safely completed without any complications. For postoperative analgesia, oral celecoxib 400 mg/day was administered until 24 hours after surgery. Thereafter, acetaminophen 3,000 mg/day and loxoprofen sodium hydrate 60 mg were administered as rescue analgesics. Postoperative hemostasis was satisfactory, and no perioperative complications were observed.
III. Discussion
A dental surgeon should have knowledge of multiple systemic diseases and have the ability to plan and perform appropriate treatment procedures in patients requiring whole body management. Herein, we report successful invasive oral treatment in the form of tooth extractions and cystectomies for the removal of intraoral infectious sources before elective cardiac surgery in a 45-year-old morbidly obese male patient with an aortic aneurysm. Aortic aneurysms are a medical emergency and can quickly lead to death. The prime consideration of the medical management for aortic aneurysms is strict blood pressure control1.
Physical and emotional stress such as anxiety or pain increases blood pressure, and patients undergoing dental treatment are generally anxious. Long surgical duration and intraoperative postural maintenance during oral surgical procedures can cause physical and emotional stress. Moreover, the use of local anesthetics with vasoconstrictors during invasive procedures such as tooth extraction and pain due to an inadequate response to infiltration anesthesia can increase blood pressure. In our patient, the stabilization of circulatory dynamics was very important to prevent the progression and rupture of the aortic aneurysm through a sudden increase in blood pressure. Initially, we considered using 3% mepivacaine without a vasoconstrictor for local anesthesia. However, 2% lidocaine with 1:80,000 epinephrine was selected for the following reasons. First, mepivacaine is believed to have weaker anesthetic effects compared to lidocaine. Second, the effects of epinephrine5 added to the local anesthetic are shortlived, lasting only a few minutes. Finally, an increase in endogenous epinephrine secretion induced by pain can increase blood pressure to a greater extent than exogenous epinephrine.
DEX is a popular sedative used in the intensive care unit for patients undergoing mechanical ventilation and has been recently approved for use in Japan in non-intubated patients requiring sedation.
Since the patient's diaphragmatic movement would be impaired with consequent breathing difficulty in the supine position because of his morbid obesity, the procedures were performed with the patient in Fowler's position. Furthermore, the patient had a mild respiratory reserve capacity and was highly sensitive to sedatives, raising the concern of sleep apnea. Therefore, it was considered appropriate to use sedatives that caused mild respiratory depression.
Aortic regurgitation is widely known to cause infective endocarditis. Montazem6 reported that infective endocarditis can be observed with high frequency in cases of oral infection. Therefore, the elimination of intraoral infectious sources before cardiac surgery, particularly valve replacement, is important7. However, severe complications are known to possible during oral surgical procedures in patients with cardiac comorbidities. Care must be taken to prevent the development of life-threatening complications in patients undergoing oral surgical procedures in order to improve the success rate of cardiac surgeries in patients with cardiac comorbidities. Intravenous sedation is extremely useful in stabilizing circulatory dynamics in such patients, and midazolam and propofol are commonly used sedatives. The former induces a dose-related settlement of the tongue root and respiratory depression, while the latter exhibits inhibitory effects on the heart and cardiovascular status. In addition to causing respiratory depression, DEX is an agonist of 2-adrenergic receptors in certain parts of the brain5, causing mild respiratory depression and exhibiting myocardial protective effects and analgesic and sedative effects3. We believe that DEX was the most suitable for our patient, in whom oral surgical procedures were associated with very high risk and might not have been possible without sedation using DEX.
In conclusion, our understanding of risk factors associated with systemic diseases enabled us to plan and safely perform oral surgical procedures with appropriate perioperative whole body management in a patient scheduled to undergo subsequent cardiac surgery.


 XML Download
XML Download