

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Early reconstruction by open reduction and rigid internal fixation has become the standard of care in the management of panfacial fractures1. Airway reconstruction and maintenance should be given equal importance during surgery. However, in cases of panfacial fracture, surgeons and anesthesiologists essentially compete for the same space. Surgeons require an unobstructed view for reconstruction and maxillo-mandibular fixation, if needed23. In such cases, oral intubation cannot be performed, as it may interfere with maxillomandibular fixation. Previously, in situations where oral and nasal intubation are contraindicated, a cricothyrotomy or tracheostomy has been used for airway maintenance4.
In 1986, Hernández Altemir5 introduced the submental route for intubation as an alternative technique for airway management in cranio-maxillofacial trauma. In this technique, a tube is passed through the anterior floor of the mouth in order to allow free intraoperative access to the oral cavity and nasal pyramid without compromising the airway in patients with skull base trauma. Submental intubation can be used for short-term airway control as an alternative to tracheostomy, but with minimal complications67.
The purpose of this study was to investigate outcomes of submental intubation in a series of patients who underwent surgical intervention for management of panfacial trauma.
II. Materials and Methods
This was a prospective clinical study conducted at the Department of Oral and Maxillofacial Surgery, Malankara Orthodox Syrian Church Medical College (Kochi, India) between October 2013 and March 2014, after obtaining clearance from the Institutional Ethics Committee (No. MOSCMC/IEC/2013/08). Seventeen patients who presented with maxillofacial trauma and for whom oral and nasal intubation was contraindicated were selected for this study. Patients with multi-organ trauma and patients requiring long-term airway support were excluded from this study.
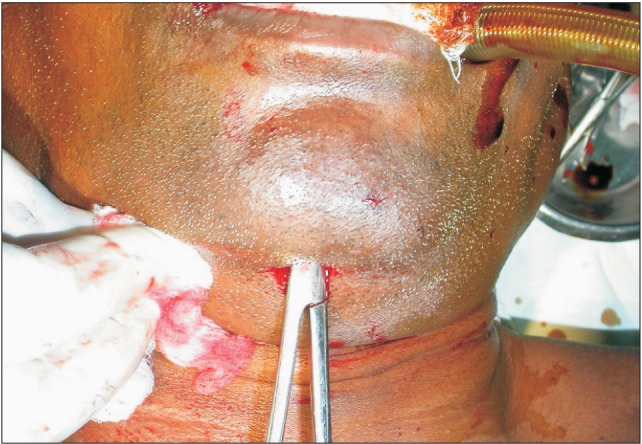
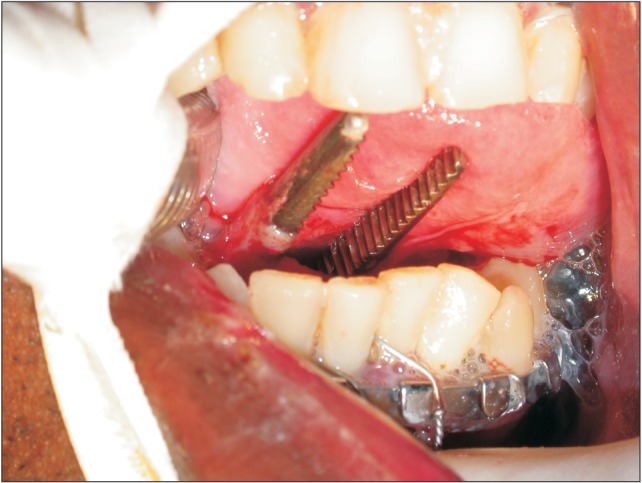
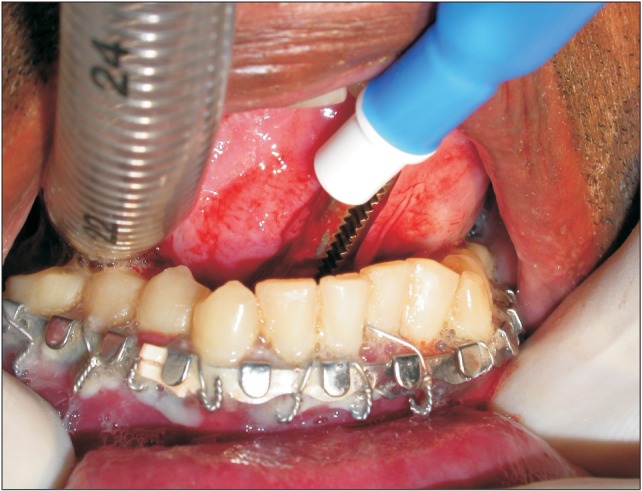
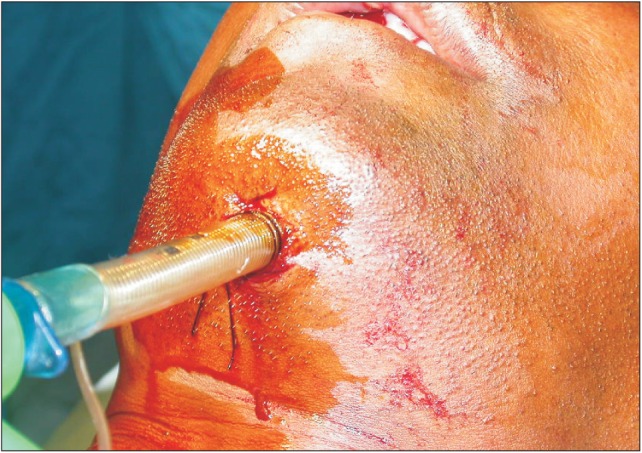
All subjects underwent orotracheal intubation by standard direct laryngoscopy after induction of general anesthesia with a reinforced cuffed flexo-metallic tube. Orotracheal intubation was then converted to submental endotracheal intubation using the following procedure. Briefly, the skin of the perioral and submental regions was prepared using betadine and alcohol. A transverse 1-cm incision was made, bisecting the midline of the face in the submental crease below the lower border of the mandible.(Fig. 1, 2) The mouth was opened, and the tongue was elevated in a superoposterior direction with a towel clip. A 1-cm midline mucosal incision was made midway between the point of reflection of the mucosa from the mandible to the floor of the mouth and the submandibular ductal papillae.(Fig. 3) The incision was then deepened inferiorly between the geniohyoid, genioglossus, and the anterior bellies of the digastric muscles. A large curved hemostat was placed through the submental incision, and the pilot tube connector was grasped and pulled through the incision.(Fig. 4, 5) The connector on the endotracheal tube was removed and then exteriorized via the submental incision. After confirmation of its adequate tracheal position by capnography and bilateral auscultation of the lungs, the tube was reconnected and secured to the skin with 1-0 silk sutures.(Fig. 6) The tube was positioned intraorally between the mandible and the tongue just above the mucosa of the floor of the mouth.
After submental intubation was complete, anatomical reduction and reconstruction using rigid internal fixation were performed using miniplate osteosynthesis. At the end of the surgical procedure, the connector was removed. The pilot tube and the endotracheal tube were passed back through the incision into the mouth, reversing the original path. The submental wound was sutured using 3-0 silk sutures. None of the patients required postoperative ventilation. Patients were reviewed at 1 week and 1 month.
III. Results
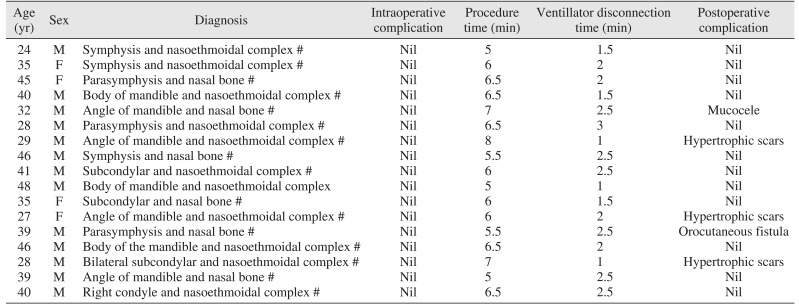
Demographic and patient clinical data are shown in Table 1. The submental intubation procedure itself did not cause any complications. In all patients, submental intubation helped to synchronize treatment of fractures without any interference from tubes. There was no need to change the method of intubation during surgery for fracture management.
The total duration of the submental intubation procedure ranged from 5 to 8 minutes, with a mean of 6 minutes. No difficulty was encountered when the tube was passed through the floor of the mouth. Disconnection and reconnection from the standard intubation to the submental intubation were performed with ease; no complicating incidents, such as accidental extubation, exposure of the wires, or loosening of the connector after reattachment, were recorded during this procedure. The period of disconnection from the ventilator ranged from 1 to 3 minutes, with a mean of 1.9 minutes. None of the patients showed any significant oxygen desaturation during the procedure. All patients were extubated in the immediate postoperative period, and none required prolonged ventilation.
In the postoperative review period, three patients developed hypertrophic scars, one patient developed orocutaneous fistula, and one patient developed mucocele.(Fig. 7) All of these complications were managed using conventional methods. There were no motor or sensory deficits recorded in any patients.
IV. Discussion
Injuries to the head and maxillofacial areas can easily jeopardize the ability to maintain the airway, and attention should first be directed to a secure airway. The development of equipment and techniques for endotracheal tube placement started after inadvertent awake placement of a tube into the trachea by Persian surgeon Desault8. Airway management for anesthetic purposes was conceived in 1871 by the famous German surgeon Trendelenberg, who adopted a method of delivering chloroform into a tracheostomy tube for human use9.
Endotracheal intubation in patients with maxillofacial trauma is challenging for both anesthesiologists and surgeons and requires good communication between them. Surgeons operating on panfacial injuries in patients with nasal or oral endotracheal intubations may interfere with the endotracheal tube while operating, which can be a potential source of infection. Nasotracheal intubation may also cause complications such as cranial intubation, epistaxis, trauma to the pharynx, pressure necrosis of the external nares, otitis media, sinusitis, sepsis, and inability to pass a tube through nasal passages101112. Nasotracheal intubation is often difficult due to deviation of the nasal septum and hypertrophy of nasal turbinates, and it can result in transfer of infection from the nose to the bronchial tree1314.
Cases of panfacial trauma occasionally call for an alternative to oral and nasal endotracheal intubation. The standard route of access has been with a tracheostomy approach for this subpopulation. However, tracheostomy can cause general, local, early, and late complications including cardiac arrest caused by stimulation of vagus nerve, post hypercapnic shock due to sudden lowering of carbon dioxide level, and aeroembolism15. Other complications include hemorrhage, subcutaneous or mediastinal emphysema and recurrent laryngeal or tracheal stricture, hemorrhage from large blood vessels caused by decubitus of vessel walls, trachea-esophageal fistula, extensive granulation, and inflammatory complications16. Cricothyroidotomy may be a useful alternative to establish an emergency airway in adult patients; however, as it is associated with significant complications, it cannot be used when prolonged ventilation is required. Additionally, cricothyroidotomy is associated with both major (death, subglottic stenosis, subglottic granulation tracheomalacia) and minor (transient hoarseness, aspiration pneumonia, pain at stoma scar, stoma site bleeding, stoma site abscess, subglottic ulceration) complications, which limits its use17.
There have been several attempts to achieve short-term airway maintenance in the literature. A simple technique of retromolar intubation was described by Martinez-Lage et al.18 and carries the advantage of no interference with occlusion in craniofacial, orthognathic, oncologic, and trauma surgery procedures. However, it has many disadvantages, including increased patient trauma, obstructive to the operative field, and long operative time.
Another alternative, the nasal tube switch technique, in which the endotracheal tube is intraoperatively shifted from the oral to nasal route, is described by González-Garcia et al.19. It carries disadvantages including risk of aspiration due to posterior nasal bleeding and potential airway compromise with need for emergency tracheostomy or cricothyroidotomy. The floor of the mouth and submental region are attractive alternative choices. Hence, attempts have been made to maintain the endotracheal tube in the midline or paramedian region. These two variations have become the techniques of choice to obtain restoration of traumatized soft tissues and bone fragments in proper approximation depending on laceration of the soft tissues and the bony architecture involved.
Endotracheal intubation with a submental route was first described by Hernández Altemir5 in 1986. This technique provides a secure airway, an unobstructed intra-oral surgical field, and allows maxillo-mandibular fixation, thereby avoiding the drawbacks and complications of oral and nasal intubation, as well as tracheostomy. This technique is also referred to in the literature as sub-mandibular intubation by Anwer et al.20 or as transmylohyoid intubation by Adeyemo et al.21. Despite the widespread use of submental intubation for other purposes, Bögi and Incze22 in 1996 recommended the use of submental intubation by a paramedian approach.
In our study, 17 patients were intubated through a submental route. The technique was found to be simple and reliable. Hypertrophic scar was found in three cases (17.6%), orocutaneous fistula in one case (5.9%), and mucocele in one case (5.9%). All postoperative complications were effectively managed. Various other complications described in the literature (e.g., trauma to the submandibular and sublingual glands or ducts, damage to the lingual and marginal mandibular nerve2324) were not experienced in our study. The findings of this study concur with the findings of Nayan et al.25 that submental intubation provides a better field of work for the oral and maxillofacial surgeon, avoids complications, and allows intraoperative maxillo-mandibular fixation in patients with nasoethmoidal complex fractures along with associated maxilla mandibular fractures without having to resort to tracheotomy.
Over time, several modifications to this procedure have been introduced. One modification introduced by Gadre and Waknis involves passage of the endotracheal tube anywhere through the mylohyoid muscle26. Another modification involves the use of two endotracheal tubes for intubation, referred to as anterograde and retrograde approaches27; this technique is believed to be superior because of the decreased chance of hypoxia. Nyárády et al.28 have suggested the "rule of 2-2-2", which describes a 2-cm-long incision, 2 cm from the midline and 2 cm medial and parallel to the mandibular margin for placement of the endotracheal tube. Mahmood and Lello29 have performed submental intubation using a preformed Sheridan tube, which has a preformed curvature that helps in positioning by conforming to the anatomy of the region. Lima et al.30 have utilized a surgical gloved finger and Adeyemo et al.21 have used a nylon tube sac to cover the proximal end of the endotracheal tube, which helps prevent entry of blood and soft tissue during its passage through the orocutaneous tunnel.
V. Conclusion
The submental route for endotracheal intubation is a simple and reliable method for short-term maintenance of airways in panfacial trauma patients because the endotracheal tube does not interfere with occlusion during fracture reduction and fixation and has minimal or negligible postoperative complications.



 XML Download
XML Download