

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Squamous cell carcinoma (SCC) in the oral cavity is a common disease that is associated with several risk factors, including smoking, alcohol use, viral infection, immunosuppression, malnutrition, chronic irritation as well as previous disease such as odontogenic cyst.
SCC associated with odontogenic cysts are extremely rare, and those arising within the jawbones occur with an incidence of approximately one or two person per thousand1.
Recently, we treated a 36-year-old male patient with SCC. He was first diagnosed with benign odontogenic cyst and underwent enucleation of right ramus of the mandible at another hospital. We further treated the same site in our hospital using segmental mandibulectomy and fibular free flap reconstruction.
The aim of this report is to introduce a clinical case of mandibulectomy and fibular free flap reconstruction in a patient with oral cancer associated with odontogenic cyst and to review the current literature.
Go to : 
II. Case Report
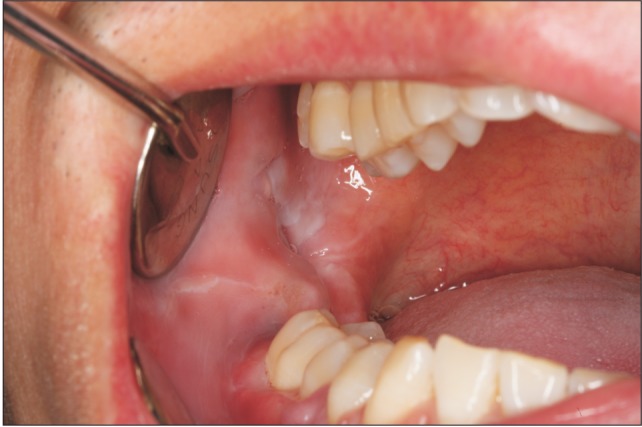
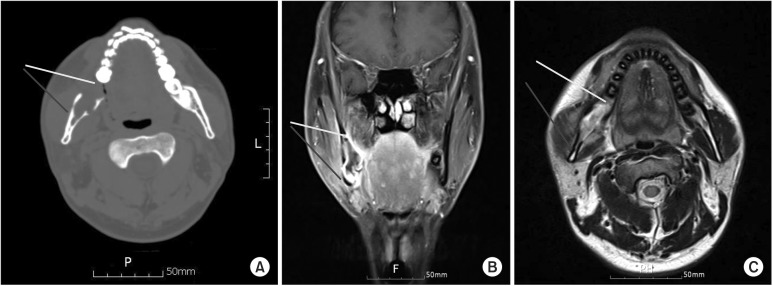
A 36-year-old male patient without specific underlying diseases visited us with intraosseous SCC in his mandibular right ascending ramus with jaw pain and limited mouth opening as chief complaints. His right mandibular pain started in May 2013, and based on the initial diagnosis of a benign odontogenic cyst, he underwent cyst enucleation in July 2013 at another university hospital. Then in the same month, based on biopsies, he was diagnosed with SCC with an odontogenic keratocyst (OKC), and he was transferred to our hospital. Based on clinical tests performed upon his arrival at our hospital, there were no specific findings in the intraoral or extraoral areas, and the patient did not complain of any severe pain or edema. Preoperative blood testing likewise revealed no specific findings. On facial examination, the patient complained of limitation in his mouth opening to approximately 20 mm and mild hyposensitivity from his right mandible to his lower lip.(Fig. 1) The preoperative radiographic findings from the cone-beam computed tomography (CT) images were a multilocular radiolucent lesion with a clear margin, a right submandibular space, and a soft tissue accessory lesion that invaded the right medial pterygoid muscle. The positron emission tomography (PET) CT images showed an increase in local uptake from the mandibular right corner and ascending ramus to the osteoclastic lesion with level of SUV max of 7.7 of PET. On magnetic resonance imaging, multiple affected lymph nodes up to levels IB, II, III, and IV were observed. (Fig. 2, 3)
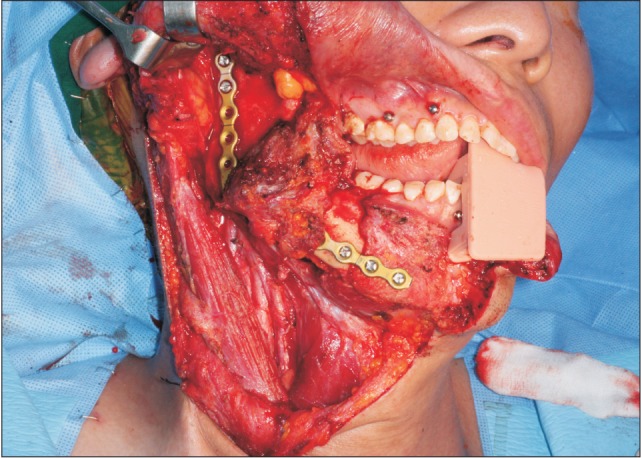
Accordingly, the patient was diagnosed with SCC caused by OKC. On August 22, tracheostomy for intubation and adequate airway control along with a wide excision with segmental mandibulectomy, supraomohyoid neck dissection (right) and reconstruction using an osteocutaneous fibular free flap were performed under general anesthesia. During the surgery, the sternocleidomastoid muscle, external jugular vein, greater auricular nerve, vagus nerve, and carotid sheath without cancer invasion were confirmed and conserved. The lower cheek flap design was used for the neck dissection, and the extended Risdon approach was used for the incision. For the segmental mandibulectomy, the incision started from the lower lip and extended to the mandibular right vestibular region, the mandibular right first molar gingiva, and the mandibular right ascending ramus. The mandible was resected from the mandibular distal right second premolar area to the mandibular inferior right condylar area. During this procedure, the mental nerve was sacrificed, and a frozen biopsy was performed. No tumor was observed in the lymph nodes. (Fig. 4,5,6) Mandibular Reconstruction Angled Plate (Stryker, Kalamazoo, MI, USA), after being bent into form on an rapid prototype (RP) model preoperatively, was used as the reconstruction plate after the plate was cut according to bone defect size.
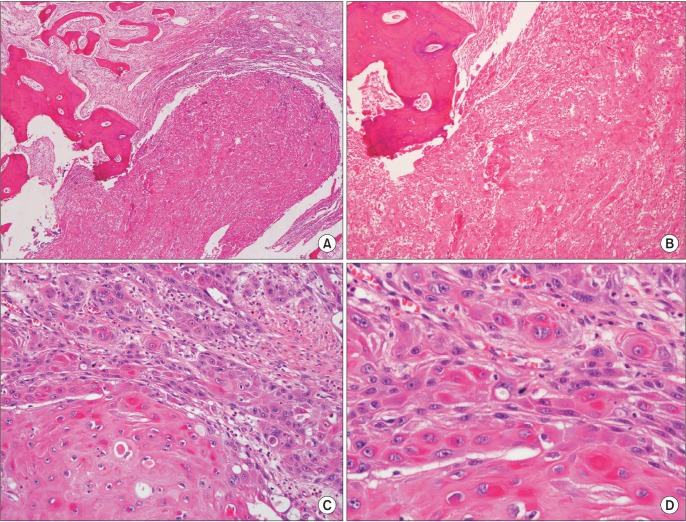
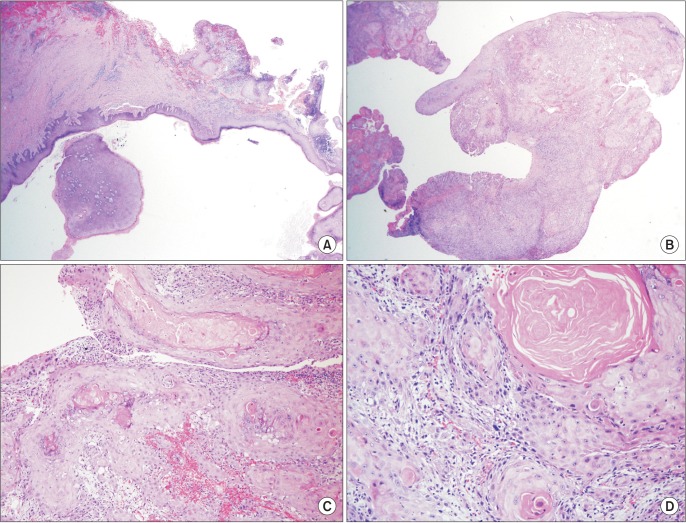 | Fig. 4Final soft tissue specimen showing squamous cell carcinoma (SCC) lesion with cyst. A. Cyst site (H&E staining, ×20). B. SCC site (H&E staining, ×20) adjacent to the cyst. C. SCC site (H&E staining, ×100). D. SCC site (H&E staining, ×200).
|
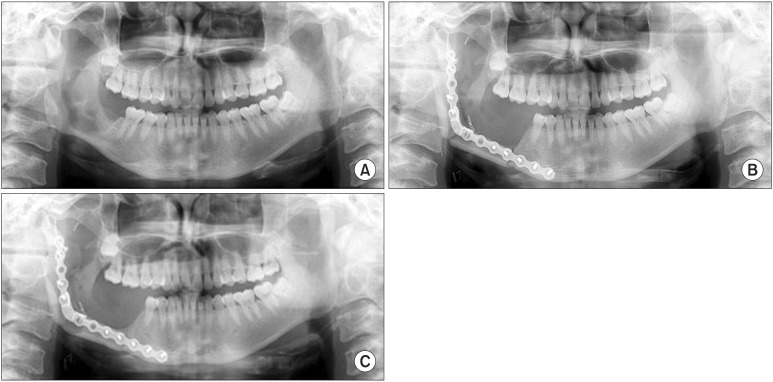
In the postoperative final main lesion biopsy, SCC was confirmed, and no metastasis was observed in the levels I, II, and III lymph nodes. Mouth-opening at six months postoperatively improved to about 40 mm, and there were no specific findings from the intraoral and extraoral PET and CT images. Accordingly, no post-operative radiographic treatments were performed, but continued follow-up was planned. The conebeam CT images obtained at eight months postoperatively yielded no specific findings. In the PET CT images obtained at 15 months postoperatively, no recurrence or metastasis in cervical lymph nodes or other organs was observed. The patient had a favorable course, clinically and aesthetically. (Fig. 7, 8) At 24 months postoperatively, iliac bone graft and implant placement were scheduled in the superior area of the fibular bone, and the reconstruction plate will be removed.

Go to :
III. Discussion
OKC is a cyst covered with thin keratinized epithelia and is the most aggressive and recurrent odontogenic cyst2. When not treated properly, it can develop into intractable disease. Moreover, it has a high probability of malignant transformation. Many maxillar and mandibular cancers are known to develop from a keratinized cyst3. Loos4 first described a malignant change in the odontogenic tumor in 1913, after which Schwimmer et al.5, Keszler and Piloni6, and Tan et al.7 reported odontogenic-cyst-induced malignant tumor cases. The mechanism of the malignant variation of the odontogenic cyst epithelia has not been clearly understood. In a study by Gardner8, 25 cases of malignant odontogenic cyst were analyzed using literature published between 1889 and 1967. When the odontogenic cyst is positioned in the maxilla or the mandible for a long time, the stratified squamous epithelia can become malignant due to chronic inflammation. There is a report that suggested that chronic inflammation of cyst epithelium could be the main predisposing factor for malignant transformation9. In the 1971 World Health Organization (WHO) classification10, there are three types of dental cancer: (1) malignant ameloblastoma, (2) primary intraosseous carcinoma, and (3) other carcinomas arising from the odontogenic epithelium, including those arising from odontogenic cysts. In the 1982 study of Elzay11, primary intraosseous carcinomas included (1) carcinomas arising from odontogenic cysts, (2) carcinomas arising from ameloblastomas, and (3) carcinomas arising from odontogenic epithelial rests of Malassez. As a result, the definitions of intraosseous carcinoma and dental cancer have been mixed. In this study, the case was diagnosed based on the WHO's odontogenic-cyst-induced squamous stratified cell carcinoma, which is different from Elzay's primary intraosseous carcinoma. The pathology report in the present case revealed an SCC lesion that arose from an initial OKC lesion. According to a study by Gardner8, odontogenic-cystinduced cancer frequently developed in the mandible (15 cases) and the maxilla (nine cases). The present case developed in the right mandible. The clinical manifestations vary according to the location, size, and grade of the cyst, but they are often subclinical in the earlier stages and found accidentally on an X-ray. With their progression, symptoms such as facial bone and facial swelling, tooth pain and mobility, mastication and mouth opening disorders, and ulcers may develop12. Marsupialization is contraindicated in the treatment of suspected odontogenic-cyst-induced cancer due to the possibility of epithelial transformation to malignancy8. Instead, removal of the nearby lymph nodes and surgical excision are recommended3,13 by Elzay11, as at least 66% of patients experience recurrence at least once. In a study by Bereket et al.14, the two-year survival rate is between 53% and 63%. According to a study by Gardner8, five of 25 patients died within 10 to 24 months after the initial diagnosis was made, but metastasis was not observed in the malignant OKC cases15. In the present case, a completely free surgical safety margin was obtained from the final specimen, and as a result of the cervical neck dissection, no metastasized cervical lymph nodes were observed. Considering the subject's age, postoperative radiotherapy was not performed. In the follow-up PET CT images at one year postoperatively, there were no metastatic findings in the lesion, cervical lymph nodes, or other organs. After the mandibulectomy, a fibular free flap and a reconstruction plate were used for immediate reconstruction for jaw function and cosmesis. The advantages of the pre-bended titanium reconstruction plate include: easy application, stability, minimal damage in the blood supply to the underlying bone, low cost, a short operative time, and postoperative aesthetic satisfaction. However, complications such as instability and delayed union, non-union, and infection due to screw loosening may develop16.
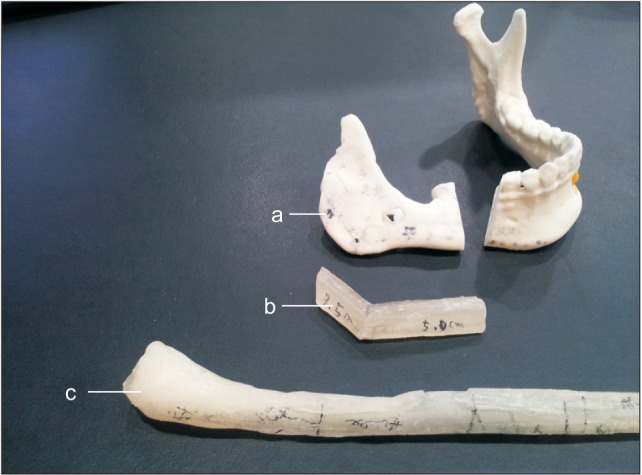
Notable in this study was the simulated operation using a skull RP model and referable fibular bone resin block for aesthetic jaw form after the wide excision and reconstruction. The free flap was designed on the subject's right ramus, and the measurements were applied to the prepared fibular bone resin block. The prepared skull RP model was used with fibular resin block for surgery simulation to save time and to reduce errors during the actual surgery. Although a preoperative guide stent and simulation surgery using computer aided design/computer aided manufacturing were not used in this study, the skull RP model, pre-bent reconstruction plate, and guided fibular resin model were used effectively for instant reconstruction during the conventional surgery. As a result, accurate postoperative facial symmetry was achieved. One and half years postoperatively, the subject shows a symmetrical profile with a high degree of self-satisfaction regarding jaw function and aesthetics without cancer recurrence. A 5-year follow-up is needed to confirm complete healing. Further studies, including a literature review on odontogeniccyst-induced cancer, may be needed in the future.
Go to :
 XML Download
XML Download