

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Basal cell adenoma (BCA) is an uncommon benign salivary gland tumor that accounts for 1% to 3% of all salivary gland neoplasms1. It is characterized by the basaloid appearance of the tumor cells and the absence of the myxochondroid tissue that is usually found in pleomorphic adenomas. The tumors have been classified into solid, trabecular, tubular, and membranous types2, and the treatments of choice are surgical excision, superficial parotidectomy, and total parotidectomy. Total parotidectomy is preferred over superficial parotidectomy for tumors in the deep portion of the parotid gland or for membranous types of BCA that tend to be multicentric, have multiple recurrences, and occasionally undergo malignant transformation3.
Here, we report a case of total parotidectomy to excise trabecular BCA in the deep portion of the parotid gland, with facial nerve preservation.
Go to : 
II. Case Report
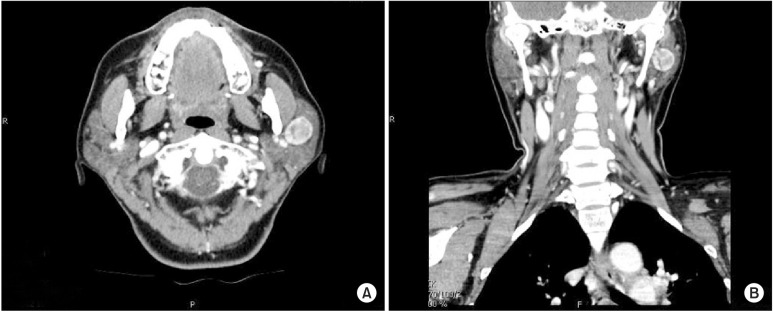
A 54-year-old Korean woman presented to the outpatient oral and maxillofacial surgery clinic at Dankook University Dental Hospital (Cheonan, Korea) in 2013 because of a six-month history of painless swelling of her left parotid gland. On physical examination, the patient showed a 1.5-cm nodule in the left pre-auricular region and a mobile mass over the deep portion of left parotid gland that had not adhered to the skin. No pathologic lymph nodes or masses were observed or palpated in the cervicofacial regions. Based on the history and physical exam, a suspected diagnosis of benign parotid gland tumor was made. Enhanced neck computed tomography images were obtained and revealed a 1.7×1.5 cm, well-defined, heterogeneously enhancing mass in the deep portion of the left parotid gland.(Fig. 1)
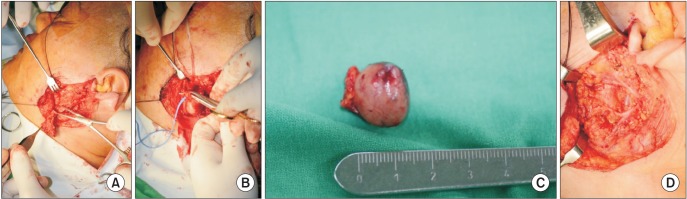
With both a clinical and radiological diagnosis of benign tumor in the deep portion of the left parotid gland, a total parotidectomy with facial nerve preservation under general anesthesia was scheduled. A modified Blair incision4 was made in the pre-auricular region (Fig. 2), and the facial nerve trunk was identified using an antegrade approach5. After the superficial portion of the parotid gland was carefully dissected to avoid facial nerve injury, the branches of the facial nerve were isolated. When the superficial portion of the parotid gland was removed, a shiny, brownish-colored mass was exposed underneath the facial nerve branches. After retraction of the nerve branches that passed into the deep lobe, the tumor mass in the deep portion of the parotid gland was excised by total parotidectomy.(Fig. 3)

Histologically, the mass in this case was shown to be a mostly trabecular type BCA tumor. Immunohistochemical examination showed that the mass was positive for p63 and high-molecular weight cytokeratine.(Fig. 4)
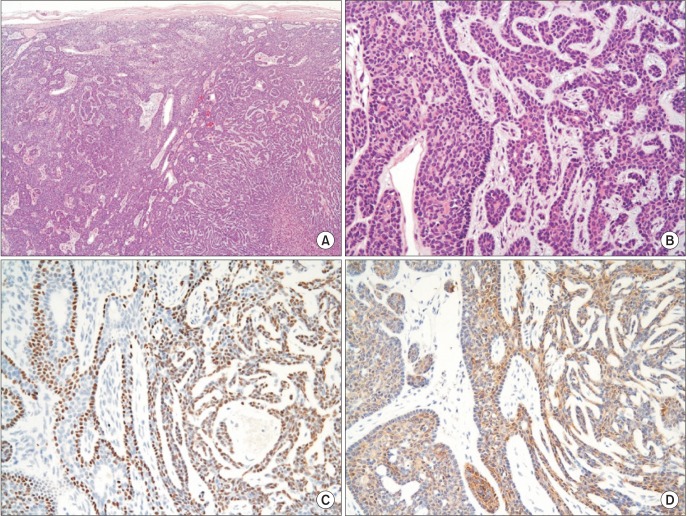 | Fig. 4A. Fibrous capsule of the tumor is surrounding trabecular tumor cell nests (H&E staining, ×40). B. Trabecular tumor cells and tumor cell nest formation (H&E staining, ×200). C. The basal cells are expressed by p63 (immunohistochemical staining, ×200). D. The luminal cells of tubular structure are stained by HMK-CK (immunohistochemical staining, ×200).
|
The patient was discharged without any complications such as facial nerve weakness or Frey syndrome, and there was no recurrence during the 24-month follow-up period.
Patients provided written informed consent for the publication of this case report along with the accompanying images.
Go to :
III. Discussion
BCA is a rare, benign epithelial neoplasm of the salivary glands that most frequently arises in the parotid gland. It is composed of relatively isomorphic basaloid epithelial cells, an abundant basal cell layer, and a distinctive basement membrane-like material. Notably, BCAs lack the myxochondroid tissue that is present in pleomorphic adenomas6. Clinically, the tumor tends to be an asymptomatic, slowly enlarging, freely mobile mass with a maximum diameter of less than 3 cm. Most authors report a greater prevalence in women, but other authors report no differences between the sexes78.
At the cellular level, the predominant tumor cell arrangement determines the type of BCA. The tumors are divided into four types by histologic pattern: solid, trabecular, tubular, and membranous. The most common type is the solid BCA9, in which round or oval tumor cells show a solid proliferation and form cell nests of various sizes. The peripheral nest cells are lined with a palisading row of tumor cells10. In the tubular type of BCA, bilayered tubular structures consisting predominantly of inner eosinophilic luminal cells and outer cuboidal cells are featured. In the trabecular type, the tumor cells are arranged in trabecular cords and occasionally form tubular lumens or intercellular canalicular slits within the trabeculae11. Membranous BCAs are composed of peripheral cell layers arrayed in a palisade fashion, and the cell layers are surrounded by excessive hyaline basal membrane material12. In this case, the tumors are mostly of the tubular and trabecular types.
For BCAs, the primary treatment is surgical excision by means of a superficial or total parotidectomy. Total parotidectomy is performed in cases in which the tumor affects the parotid gland because BCA can be unencapsulated. However, in the minor salivary glands of the oral mucosa, extracapsular excision is performed to treat BCAs3. Total rather than superficial parotidectomy is preferred in the membranous type of BCAs because the membranous type tends to be multicentric, have multiple recurrences, and occasionally undergoes malignant transformation1213.
When performing a total parotidectomy, surgeons endeavor to preserve the facial nerve, which is challenging because the deep lobe of the parotid gland is beneath the facial nerve and its branches14. Thus, many surgeons perform superficial rather than total parotidectomies in patients with potential malignant transformation or primary superficial cancer of the parotid gland. However, Kidd15 reported a series of 105 patients with pleomorphic adenoma that were treated with total conservative parotidectomy, and no cases of permanent paralysis were seen. In addition, Laccourreye et al.16 studied 229 cases of primary benign pleomorphic adenoma of the parotid gland and found facial nerve dysfunction to be no more common after total conservative parotidectomy than after superficial parotidectomy. Although Gaillard et al.17 reported that total parotidectomy was associated with a significantly higher incidence of temporary facial nerve dysfunction than was superficial parotidectomy, there was no permanent facial nerve dysfunction in either total or superficial parotidectomy.
Thus, in the absence of a preoperative biopsy, conservative total parotidectomy with facial nerve preservation is recommended for suspected BCA because membranous BCAs can occasionally become malignant.
Go to :
 XML Download
XML Download