

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
When dentists and rhino-laryngologists choose minimally invasive endoscopic procedures, a sound knowledge of the normal anatomy and variations in the anatomy of the maxillary sinus is necessary. Preprosthetic surgeries, like maxillary sinus floor augmentation through a lateral antrostomy, gained popularity in restoring functional dentition in the posterior maxilla1. The most common complication reported following these surgeries is sinus mucosa perforation (Schneiderian membrane), with an incidence of 35% according to Rosano et al.2 and 10% to 56% according to Pikos3. Anatomical variations, such as the presence of maxillary sinus septa (MSS), increase the chances of membrane perforation leading to profuse bleeding during implant therapy. MSS can obstruct proper visualization of the maxillary cavity and can also hamper the preparation, elevation, and inversion of the bony window along the anterolateral wall during sinus floor augmentation2,3,4.
Underwood4 first reported MSS (antrum of Highmore) in 1910. He described the septa arising between the areas of two adjacent teeth from the floor of the sinus, located in three specific sections. Underwood4 classified them into anterior (between the second premolar and first molar), middle (between the first and second molar), and posterior (distal to the third molar) septa depending upon their location4. It was only recently that the maxillary antrum was explored on radiographs and three-dimensional computed tomography (CT) images, due to the increased use of osseointegrated implants5,6. Currently, there are no cadaveric studies of MSS in our population documented in the literature. Hence, this study was planned to evaluate the incidence, location in different anatomical planes, and height of MSS in dentate and edentulous maxillae.
II. Materials and Methods
The study was carried out in Department of Anatomy, Rural Medical College, Pravara Institute of Medical Sciences (Loni, Maharashtra) during 2012-2014. Permission from the institutional ethical committee of Pravara Institute of Medical Sciences was granted before starting this project. We examined 210 maxillary sinuses that were available in our department. The cadavers were fixed in 10% neutral formalin and were partially dissected by medical students. The anatomic specimens belonged to subjects ranging in age from 45 to 80 years (mean age, 63 years). All included cadavers were free of any sign of maxillary sinus deformity. Specimens with evidence of pathology, such as fractures, inflammation, cysts, or tumors were excluded from the study.
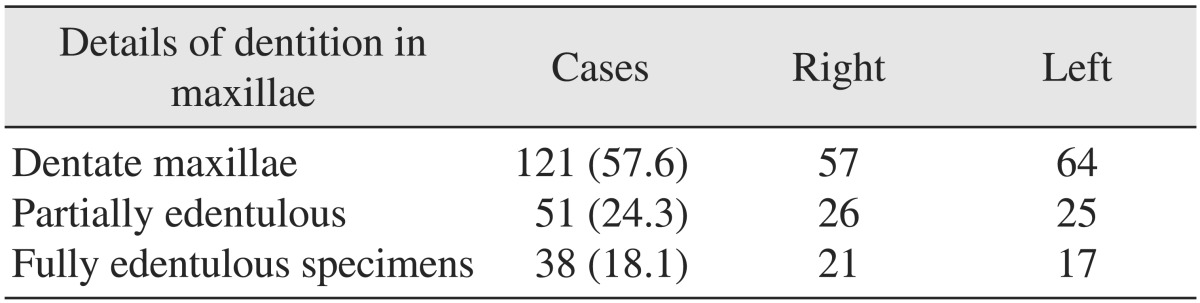
Midsagittal cuts were made with an electric band saw, dividing the skulls into two halves. The cases were divided into two groups, a non-atrophic/dentate segment and an atrophic/edentulous segment, as suggested in Table 1. The location of the maxillary ostium was noted in relation to the semilunar hiatus, and the distance between the maxillary sinus ostium (MSO) and nasal floor was measured with a sliding vernier caliper by keeping the head in Frankfurt's plane. Consequently, the sinus was explored from the medial aspect by dissecting the three nasal conchae and the lateral wall of the nasal cavity. Thus, direct visualization of potential septa within the alveolar recess of the antrum was made possible.
MSS less than 2.5 mm were not taken into consideration. The orientations of the MSS in the anatomical plane were studied in detail. The heights of the septa were measured from the sinus floor and from the wall on which they arose to the more inferior point of the two possible sides of the septum.
III. Results
All the bony septa observed were incomplete.
2. Distance between the maxillary sinus ostium and the adjoining anatomical landmarks
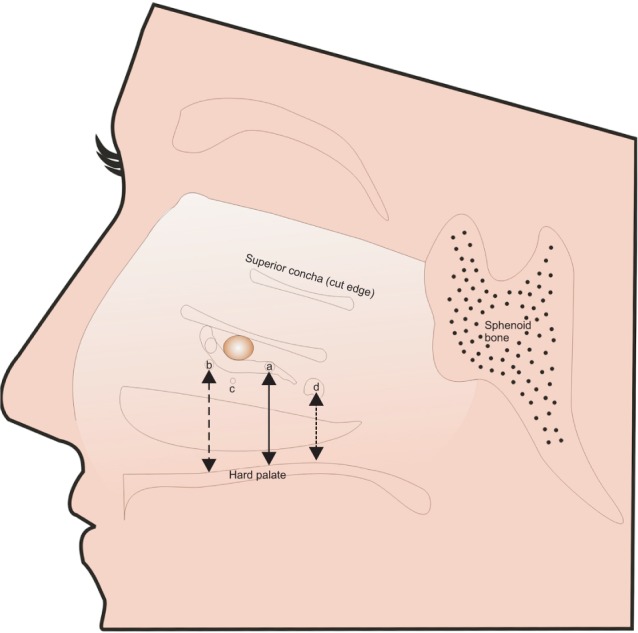
The linear distance between the inferior most point of the maxillary sinus floor and the ostium in the semilunar hiatus was 44±5 mm on the right and 43±4 mm on the left side.(Fig. 1) The distance between the nasal floor and the maxillary ostium was 36±4 mm on the right and 37±5 mm on the left side. Also, the distance between the nasal floor and the maxillary sinus floor was 8±2 mm on the right and 7±1 mm on the left side. In 165 of 210 cadavers (78.6%), the MSO was located in the posterior portion of the semilunar hiatus.
3. Incidence and location of MSS in different anatomical planes
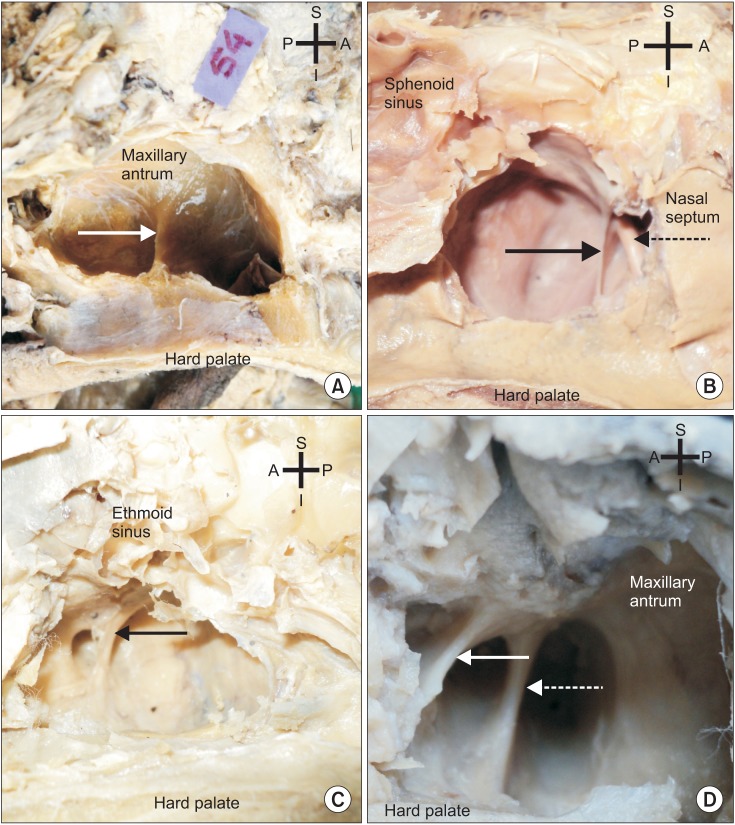
A total of 59 incomplete septa were observed in 210 maxillary specimens. Single MSS were found in 53 cases. In three specimens, two septa were observed in a single sinus cavity. Interestingly, two of the septa were found in the sagittal plane only.(Fig. 2. D)
The MSS were oriented in two anatomical planes, coronal and sagittal. The coronally-oriented MSS were further categorized according to their origin:
Category I, MSS arising from the floor of the sinus were most common and transversely oriented. There were 33 septa (55.9%) located in the middle (between the first and second molar) and posteriorly (distal to the third molar) to the maxillary antrum.(Fig. 2. A) We did not find MSS arising from the anterior part of the sinus floor.
Category II, MSS originating from the lateral wall of the maxillary sinus, located between the first and second molar tooth (middle in location).(Fig. 2. B) These MSS were dividing the cavity into two incomplete anterior and posterior compartments and were found in nine cases (15.3%).
Category III, septa located in the antero-superior quadrant of the maxillary sinus were observed in 19 specimens (32.2%). Anatomically, the septa were oriented sagittaly, with branches of the infraorbital nerve (ION) embedded in them. They were present individually (Fig. 2. C) or found as a pair (Fig. 2. D) in the antrum. Incidences and percentages are shown in Table 3.
In seven specimens, two sagittal septa were observed in one sinus cavity, and the anterior superior alveolar nerve branch of the ION was seen in three (one right and two left) of these septa.(Fig. 2. D) The Schneiderian membrane was tightly adhered to the internal aspect of the sinus cavity, as well as to all the sinus septa.
4. The height of MSS in various anatomical planes
The height of the MSS was variable in the different anatomical planes.
MSS located in the coronal plane: the mean height of the category I MSS arising from the floor was 9.7±1.62 mm and 10.3±1.78 mm on the right and left side, respectively.(Fig. 2. A) The category II MSS reached their maximum height on both the right and left side. The mean height observed was 12.7±3.29 mm on the right and 14.1±3.60 mm on the left side.(Fig. 2. B) The category III MSS were smallest in dimension, as shown in Table 4.
5. Separate bony canal for the infraorbital nerve and its branches
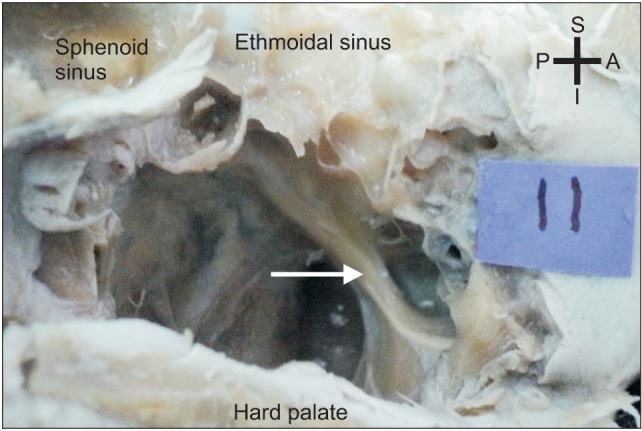
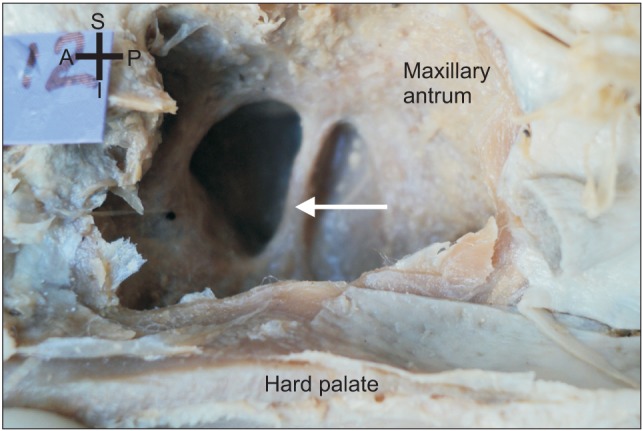
In four specimens, we found a separate canal for the ION within the maxillary antrum.(Fig. 3) In three of these specimens, the anterior superior alveolar nerve, which is a branch of the ION, was embedded within the MSS. Interestingly, we found that the middle superior alveolar nerve, after originating from the ION, traversed in a bony trabecula directly in the middle of the sinus, extending from roof to floor.(Fig. 4)
IV. Discussion
Knowing the distance between the maxillary sinus floor and the normal ostium helps in selecting the appropriate volume of augmentation material during pre-implantological sinus floor preparation. The most commonly used Branemark implants measure 3.75 mm and 13 mm in diameter and length, respectively, and require a distance of 20 mm or more in the molar region to be successfully implanted7. In the present study, the linear distance between the inferior most point of the maxillary sinus floor and the normal ostium in the semilunar hiatus was found to be greater than the reports of previous studies, 44±5 mm on the right and 43±4 mm on the left side. Specifically, Uchida et al.7 and Gosau et al.8 mentioned the mean distance to be 28.5±5.08 mm and 25.6 mm, respectively, and these distances are quite sufficient to allow preprosthetic implant placement.
The normal MSO was at an usual location (posterior part of the semilunar hiatus) in 165 of 210 specimens (78.6%). In the remaining 45 cases (21.4%), the ostium was variably located in a position inferior to the semilunar hiatus.(Fig. 1) The distance between the nasal floor and the ostium was 36±4 mm on the right and 37±5 mm on the left side, but this distance varied in the presence of accessory maxillary ostia. May et al.9 reported the distance between the nasal floor and the maxillary ostium to be 40 mm. In healthy specimens, the MSO is located very close to the orbital floor, and hence, the knowledge of the exact location becomes mandatory to effectively and safely perform functional endoscopic sinus surgeries4,6,8,10,11.
The location of the MSS is described in different ways by previous authors. The classical theory of sinus septa was introduced by Underwood4 and was later followed by Kim et al.5, who described the location of septa as anterior, between the roots of second premolar and first molar, middle, between the roots of first and second molars, and posterior, distal to third molar roots. Recently, Maestre-Ferrín et al.6 divided the sinus floor into the anterior area, corresponding to the premolar area, middle area, corresponding to the area between the superior and first molar, and posterior area, corresponding to the area of the second molar. The sinus division by Maestre-Ferrín et al.6 was accomplished by drawing two straight lines perpendicular to the floor of the sinus equidistant from the anterior and posterior walls of the sinus. Thus, they obtained the anterior, middle, and posterior regions6,10. Controversy exists about the division of the maxillary sinus cavity into various compartments, and hence, the location of the septa is classified differently according to different authors.
The present study evaluated the MSS in an Indian population for the first time. Our findings regarding the location of the MSS are in agreement with Kim et al.5 and Rosano et al.2, who also encountered more septa in the middle region of the sinus cavity, as shown in Tables 5 and 62,4,5,6,8,10,12. Their results, in addition to our results, are in contrast to Gosau et al.8 and Underwood4, who found MSS to be more numerous in the posterior portion of the sinus. These variations may be due to differences in chewing habits in different geographical areas.
Previously, the MSS were only described arising from the maxillary sinus floor. Recently, Rosano et al.2 reported the existence of MSS in two anatomical planes (sagittal and transverse). They found 20 MSS (33.3%) in 60 sinuses. Fourteen septa were sagittal and six were in the transverse plane. One septa per sinus was found to be oriented in the sagittal plane, either anteriorly or in the middle, and all transverse septa were located in the posterior region. Study by Rosano et al.2 found the sagittaly oriented septa in anterior and middle region and transverse septa in posterior part of maxilla. In the present study, we encountered coronal septa in middle and posterior regions and sagittal septa in anterior part. Jung et al.12 detected more MSS in posterior portion of maxillary sinus in comparision to anterior region in their radiographic study with the help of panorama CT. Whereas in the present study, the coronal septa were located in the middle or posterior locations, and the sagittal septa were all anteriorly placed.(Table 3) In this study, we found the septa arising from the floor, lateral wall, and also along the antero-superior portion of the maxillary antrum. The cortical bone septa, which arise from the floor (category I), complicate the inversion of the bone plate and elevation of the Schneiderian membrane during sinus floor augmentation procedures. During endoscopic surgery in the maxillary sinus via transnasal approaches, pronounced septa may hamper visibility, making a transoral route preferrable2,8. The category II and III MSS, which have considerable height, should be considered when facial surgeries and lateral antrostomies are being planned. In cases where the ION was seen in sagittaly-oriented MSS, accidental injury during sinus or facial procedures may lead to ION palsy2,5,7.
Mailleux et al.13 reported a rare anatomical variant in the form of a bony septum crossing the upper part of the maxillary sinus with the ION located within this septum. In two patients, the ION was present in a canal running through the upper part of the maxillary septum. In these cases, any surgical attempt to breakdown this septum would result in ION palsy, with permanent paresthesias in the maxillary region. The ION is also liable to injury after facial trauma, resulting in a similar presentation of paresthesias. We also observed the passage of the ION and its branches within the center of the maxillary antrum within thin bony trabeculae. Therefore, radiologists and dentists should be aware of these anatomical variations in the maxillary sinus. Rare anatomical variations like the presence of a bony trabecula containing the middle superior alveolar nerve in the center of the maxillary antrum should also be kept in mind by radiologists for proper imaging interpretation and by anesthesiologists because complete anesthesia cannot be achieved by targeting the ION just in the infraorbital foramen, as some of the fibers escape through this bony trabecula13.
Developmentally, these MSS may be primary or secondary. Neivert stated that the "primary septa" were derived from finger-like projections produced by embryonic outpouchings of the ethmoidal infundibulum where the contiguous wall failed to resorb during development14. Chanavaz15 reinforced that the congenital septa (primary septa) develop during the growth of the mid part of the face and are present in all regions of the maxillary sinus. The "secondary septa" are produced due to tooth loss and atrophy of the maxillary sinus bone, leaving an irregular bony crest on the maxillary floor16. It is difficult to label a septum primary or secondary without radiographic history of the sinus in question, but it can be concluded that septa located apical to the dentate regions are primary (developmental) and those located apical to the edentulous maxilla can be either primary or secondary15. Shibli et al.10 mentioned that pneumatization of the maxillary sinus after the fall of teeth leads to formation of MSS in edentulous maxilla. Septa vary in number, thickness, and length, and may influence the placement of dental implants and sinus augmentation procedures.
The range of anatomical variations in incidence, location, and height of the maxillary septa are wide. Therefore, all the surgical procedures in and around the maxillary sinus should be preceded by adequate radiographical examination and its efficient assessment.
V. Conclusion
Knowledge of location of maxillary sinus ostium is mandatory for the rhinologist for drainage of secretions in maxillary sinusitis. The morphological details of maxillary sinus septa, particularly their location and anatomical planes, will guide dentists in performance of safe implant surgeries. The maxillary antrum septa of category I and II may complicate the procedure of inversion of bone plate and elevation of sinus membrane during maxillary augmentation surgeries. The category III septa observed in the sagittal plane were embedded by one of the branches of the infraorbital nerve in it, and if accidentally cut will lead to infraorbital nerve palsy in maxillary sinus surgeries.





 XML Download
XML Download