

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
The conventional treatment for osteochondroma in the mandibular condyle is total condylectomy1234. However, this procedure can result in extensive and unnecessary tissue removal, which may necessitate secondary reconstruction using a costochondral graft or a total temporomandibular joint (TMJ) replacement25. Wolford et al.26 reported successful outcomes using conservative condylar resection, which involves resection of the condyle immediately below the head and above the neck, followed by reshaping the remaining condylar neck and repositioning the articular disc; they named this technique conservative condylectomy. Recently, condylectomy has been widely used as a conservative surgical procedure, and numerous surgical techniques followed by orthognathic surgery have been introduced to correct facial asymmetry in patients24567. Although conservative condylectomy alone has corrected facial asymmetry in some cases, there are far fewer reported cases of conservative condylectomy alone compared with reported cases using total condylectomy or combined orthognathic surgery189.
Herein, we report our experience with conservative condylectomy alone, without subsequent orthognathic surgery in five patients with facial asymmetry secondary to condylar osteochondroma. All patients showed satisfactory and stable long-term outcomes.
Go to : 
II. Case Report
We evaluated 12 patients with a histological diagnosis of condylar osteochondroma among patients who underwent surgery at our institution from 2004 until 2013.
Of these 12 patients, seven were excluded: three were followed for less than a year, two underwent simultaneous orthognathic surgery because of unilateral osteochondroma with hemimandibular hyperplasia, and two underwent total TMJ replacement. Ultimately, five patients were included in this report. Patient characteristics and outcomes are summarized in Table 1. This study was approved by Institutional Review Board of Gangnam Severance Hospital (IRB #3-2015-0047). Patient consent was obtained.

Table 1
Patient characteristics and outcomes
![]()
All patients were admitted to the hospital with a chief complaint of facial asymmetry, malocclusion, and TMJ pain. Clinical examination revealed deviation of the tip of the chin from the facial midline toward the unaffected side and a severe lip cant. Computed tomography revealed the presence of a mass in the mandibular condyle. Based on clinical and radiographic examination, a diagnosis of condylar osteochondroma was made.
All patients underwent surgery under general anesthesia using a preauricular approach from the affected side. The tumor mass was resected by exposing the condyle, and the remaining intact condyle was reshaped. The articular disc was also repositioned. For occlusal stabilization after surgery, intermaxillary traction was applied using a skeletal anchorage system with 1/4-inch rubber elastics that required a miniscrew10. Occlusion in two patients did not require additional orthodontic treatment after surgery, while two other patients required minimal orthodontic treatment using a mini-screw or a temporary occlusal resin stop for the correction of residual posterior malocclusion. In one patient, who had dentures prior to surgery, new dentures were fabricated to restore normal occlusion after surgery. Physiotherapy, under the supervision of a surgeon, was necessary for all patients and included mouth opening, protrusive, and lateral excursive movements.
All patients were satisfied with their facial symmetry after surgery and did not desire additional orthognathic surgery. Furthermore, the amount of mouth opening, TMJ pain and sound, and malocclusion improved in all patients. Radiographic and clinical examination was performed during the postoperative follow-up period, and all patients showed stable outcomes with no lesion recurrence at the last follow-up (average follow-up, 42 months).(Table 1, Fig. 1,2,3,4)
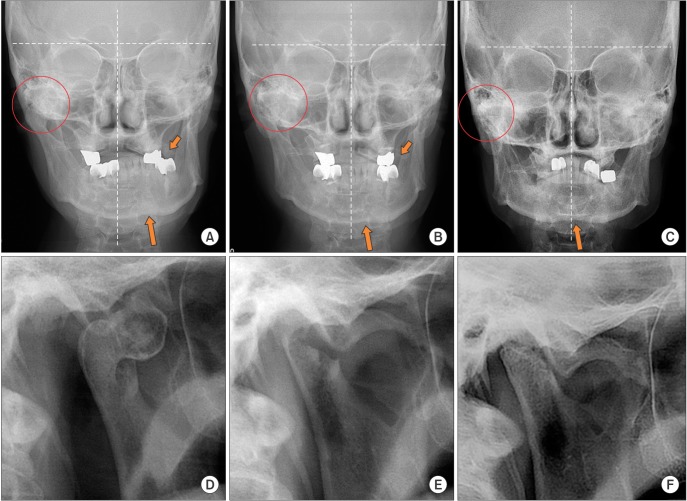 | Fig. 1Posteroanterior (A-C) and panoramic radiographs (D-F) of the right condyle of patient 1 (circle, right condyle; long arrow, menton; short arrow, crossbite of left molars). A, D. Preoperative radiographs show the overgrowth of the right condyle, deviation of the menton, and crossbite. B, E. Radiographs obtained on postoperative day 1. C, F. Radiographs obtained 80 months after surgery show appropriate facial symmetry with remodeling and recovery of the contour of the remaining condylar neck. There are no signs of lesion recurrence.
|
 | Fig. 2Photographs of occlusion in patient 2. A. Preoperative photographs show the occlusion in patient 2. Dental midline shift and left-sided crossbite are apparent. B. Photograph obtained on postoperative day 1. C. Photographs obtained 85 months after surgery show favorable occlusion.
|
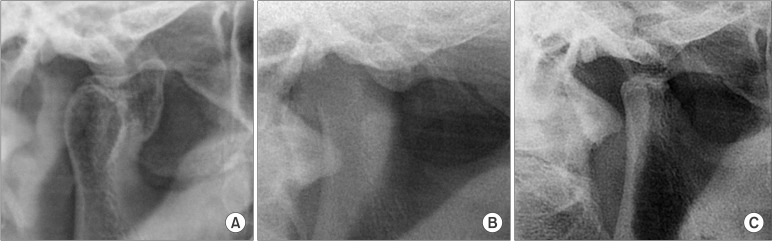 | Fig. 3Panoramic radiographs of the right condyle in patient 2. A. Preoperative radiograph. B. Radiograph obtained on postoperative day 1. C. Radiograph obtained 85 months after surgery.
|
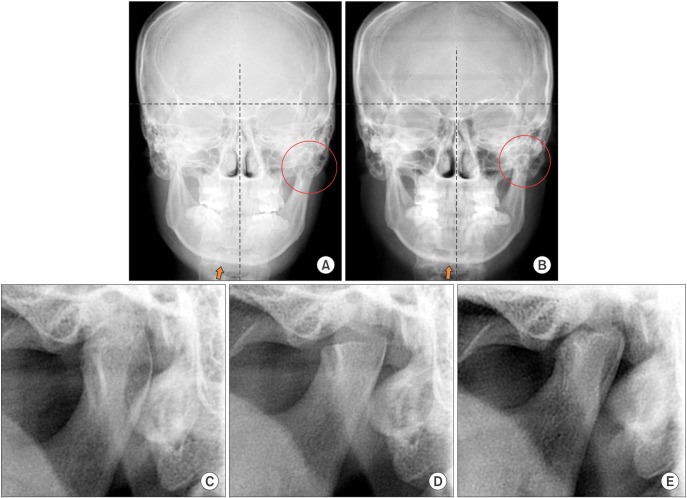 | Fig. 4Posteroanterior (A, B) and panoramic radiographs (C-E) of the left condyle in patient 3 (circle, left condyle; arrow, menton). A, C. Preoperative radiographs show hypertrophy of the left condyle and deviation of the menton. D. Radiograph obtained on postoperative day 1. B, E. Radiographs obtained 18 months after surgery show appropriate facial symmetry and remodeling and recovery of the contour of the remaining condylar neck.
|
Go to :
III. Discussion
Osteochondroma, which is an exophytic growth from the perichondrium that develops in cortical bone, accounts for 8% to 15% of all primary bone tumors and 35% to 50% of all benign tumors1711. It frequently occurs elsewhere in the skeleton, but is rare in the craniofacial region12611. The coronoid process and condyle are frequent sites of osteochondroma involvement in the mandible81213. Osteochondroma in the mandibular condyle can continue to proliferate in a patient' s skeletal bone even after cessation of bone growth, and the age of occurrence ranges from 13 to 70 years (average age, 38.4 years)1.
Generally, osteochondroma in the condyle grows gradually, with a slow manifestation of the accompanying clinical signs and symptoms. Malocclusion due to unilateral open bite and contralateral crossbite are common, making mastication or speaking difficult. In addition, hypomobility of the TMJ, such as limited mouth opening, can occur. Some patients also complain of discomfort caused by TMJ pain or sound. Progressive facial asymmetry is a typical feature, and bowing of the lower border of the mandible due to vertical displacement, unilateral mandibular elongation, concave facial profile, a midline shift, and chin asymmetry can also appear. Occasionally, maxillary arch canting or teeth inclination can occur due to compensatory vertical growth of the maxilla. Hearing loss occurs in rare cases156.
Conventionally, a total condylectomy is performed to remove the affected condylar process completely, and an iliac crest graft, the lateral head of the clavicle, and a costochondral graft are used to reconstruct the postsurgical defects214. However, even costochondral graft, which is the most appropriate condylar reconstruction technique, has been criticized for its unpredictable growth and resorption2715. Total joint prosthesis placement and distraction osteogenesis have also been attempted to overcome unpredictable growth and donor morbidity15.
Recently, conservative condylectomy has been used to preserve the condyle and to allow normal function2. Furthermore, as alternatives to grafting after radical excision, numerous surgical procedures that correct facial asymmetry without additional graft harvesting have been introduced5616. Although conservative condylectomy alone has corrected facial asymmetry in some cases, the number of such cases is significantly lower than cases treated by total condylectomy or combined orthognathic surgery189.
In the present cases, the mass was removed and mandibular asymmetry was corrected by using conservative condylectomy alone, with stable long-term results. The mass was confirmed and was removed using a preauricular approach. The condylar stump that remained after excision was recontoured for functionality as a "new" condyle, and the articular disc was repositioned. A patient's deviated chin, midline and malocclusion were mostly corrected after conservative condylectomy. After surgery, additional treatments, such as intermaxillary traction using skeletal anchorage system with 1/4-inch rubber elastics, were conducted in all patients to improve occlusion10.
Conservative condylectomy allows for appropriate resection of the condylar osteochondroma, preserves the native condyle and articular disc, and is not associated with donor site morbidity due to the lack of additional grafting26. However, conservative condylectomy alone is not always an appropriate method for treating osteochondroma. For example, patients with severe facial asymmetry with cant of the maxilla from compensatory growth caused by osteochondroma or with hemimandibular hyperplasia require subsequent orthognathic surgery. Moreover, when conservative condylectomy alone cannot completely remove the growing mass because of invasion below the condylar neck, appropriate radical resection is required to achieve stable results without recurrence. In addition, if the mandibular vertical height decreases after tumor removal, condylar reconstruction with bone grafting or alloplastic total TMJ replacement may be required17.
In conclusion, the findings from these cases suggest that conservative condylectomy without subsequent orthognathic surgery is a good treatment option for condylar osteochondroma in patients with appropriate indications.
Go to :
 XML Download
XML Download