

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
Oral cancer is the eleventh most common cancer in the world1. Its incidence is predominantly high in northern India, other Asian countries, and in certain places in the western hemisphere. It has been reported that 90% of oral cancers in India among men were attributable to chewing and smoking habits. In India, the age-standardized incidence rate of oral cancer is 12.6 per 100,000 people2. Oral squamous cell carcinoma develops through a multi-step process of genetic, epigenetic, and metabolic changes resulting from exposure to carcinogens3. The initial presence of a precursor cell subsequently developing into cancer is well established in oral cancer4. Oral leukoplakia, submucous fibrosis, and lichen planus are major known precursor lesions. The prevalence of malignant transformation of oral lichen planus is around 0.5% and approximately 1% for leukoplakia5. Ability to clinically predict malignant transformation is difficult and routine histopathological diagnosis has limited prognostic value. Despite advanced technologies for early detection of oral precancerous and cancerous lesions, there are limitations for its use, including that diagnosis is essentially subjective, all lesions exhibiting dysplasia do not eventually become malignant and may even regress, and carcinoma can develop from lesions in which epithelial dysplasia was not diagnosed on previous biopsies67. Therefore, it is necessary to develop other methods for predicting the malignant potential of premalignant lesions and preventive measures7.
Recently, strong evidence has suggested that the nuclear factor-κB (NF-κB) signaling pathway plays a critical role in carcinogenesis, protection from apoptosis, and chemoresistance in a number of cancer types, including head and neck cancer, breast cancer, hepatocellular carcinoma, and gastric cancer89101112. Recently, accumulating evidence has suggested that the NF-κB-dependent cytokine levels are elevated in saliva and tissue specimens of patients with oral premalignant lesions13. Furthermore, different cytokines can act as diagnostic tools for detecting oral cancerous and precancerous lesions and conditions. Interleukin (IL)-6 levels are significantly increased in oral cancer patients14151617. It has been evident that different cytokines are expressed by cancerous cells, the most common of which include tumor necrosis factor alpha (TNF-α), IL-1, IL-6, and IL-8151617. Limited studies were conducted on roles of TNF-α, IL-6, and IL-8 in oral precancer and cancer151617. The local and systemic nature of these responses suggests the hypothesis that cytokines with proinflammatory and proangiogenic activity are produced by precancers and cancers and could contribute to the pathogenesis of oral malignancy. In this study, we hypothesized that salivary and serum TNF-α, IL-6, and IL-8 levels could be elevated in oral precancerous lesions and conditions. To test this hypothesis, this study was conducted to analyze the concentrations of TNF-α, IL-6, and IL-8 in oral precancer using saliva and serum samples.
II. Materials and Methods
1. Eligibility
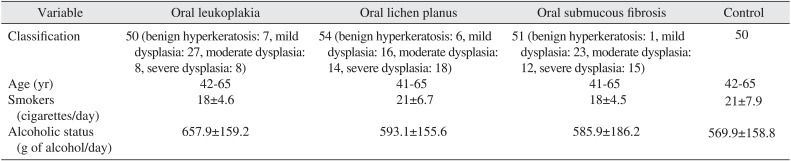
CConsecutive patients clinically and histopathologically confirmed as having oral lichen planus lesions, oral leukoplakia, and oral submucous fibrosis were recruited for this study from Baba Nidhan Singh Hospital, Punjab, India, based on the definition of oral cancer and precancerous lesions by the World Health Organization9. Healthy normal patients served as the control group. Demographic characteristics of patient and controls characteristics were mentioned in Table 1. The mean and standard deviation of smoking and alcoholic status was also ascertained. Patients and healthy subjects with matched periodontal status were selected.
All subjects had neither a smoking history nor any visible oral lesions under careful examination. Additionally, they had not received any treatments for the oral lesions within 90 days prior to the specimen collection, and had no history, symptoms, or signs of systemic infections or other diseases.
Histopathological diagnosis was made by a single oral pathologist. This study was approved by the ethical committee of Baba Nidhan Singh Hospital, Punjab, India and informed consents were obtained from all subjects as per the Declaration of Helsinki.
2. Evaluation during study
For each sample, 1.0 mL of supernatant was used for the enzyme-linked immunoassay (ELISA) cytokine assay by using the human ELISA kit for TNF-α, IL-6, and IL-8 (R&D Systems Inc., Minneapolis, MN, USA), according to the manufacturer's instructions.
3. Salivary and serum cytokine measurements
Blood and serum samples were drawn between 9:00 and 10:00 AM from all subjects. Serum was separated from blood cells by centrifugation at 1,000 g for 5 minutes. The whole unstimulated saliva was collected between 9:00 and 10:00 AM. The subjects abstained from eating and drinking for at least 2 hours prior to the sampling. All subjects were requested to swallow first, tilt their head forward at more than 45°, and then expectorate saliva (10 mL) into a sterile centrifuge tube without swallowing for 4 to 5 minutes. The saliva was then centrifuged for 25 minutes at 3,500 g, and the clarified supernatants were separated into 2.0 mL aliquots. All samples were immediately frozen at -60℃ for future use. Prior to assays, the serum or saliva supernatants were allowed to thaw completely at room temperature for two hours. For each sample, 1.0 mL of supernatant was used for the ELISA cytokine assays, using the human ELISA kit for TNF-α, IL-6, and IL-8, according to the manufacturer's instructions. The absorbances of the samples at 492 nm for TNF-α, IL-6, and IL-8 were measured with a spectrophotometer (Sirio; Seac, Florence, Italy). A standard curve was organized by plotting the absorbance value of the standards versus corresponding concentrations. The concentrations of the cytokines in the sample were then determined by extrapolating from the standard curve. Tests were run in duplicate to check reliability. Protein contents were expressed in pg/mL. The inter-assay coefficient of variation was 3.0% to 4.5% and the intra-assay coefficient of variation was 2.5% to 4.2%.
Data normality was evaluated by Smirnoff Kolmogorof's test. The Kruskal Wallis test was utilized for comparisons between the groups. Mann-Whitney test for comparisons performed to detect any differences between the two groups. A P<0.05 was considered as statistically significant. All data was statistically analyzed using the SPSS version 11.5 (SPSS Inc., Chicago, IL, USA).
III. Results
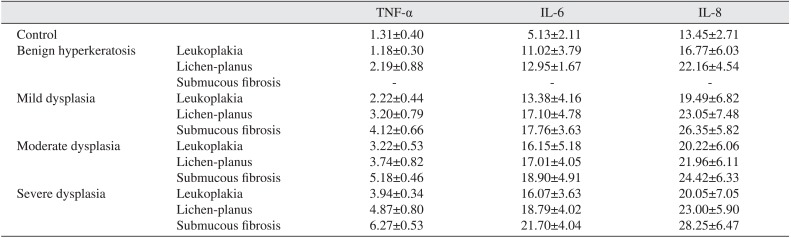
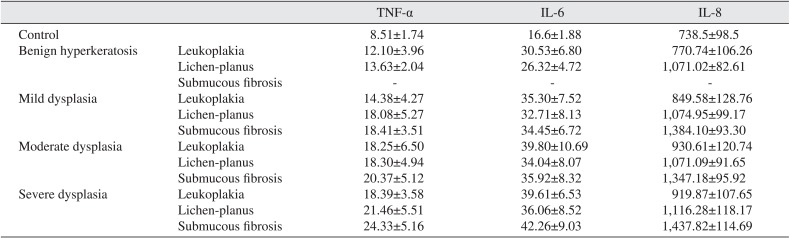
The demographic characteristics of patient and controls are mentioned in Table 1. The levels of serum and salivary TNF-α, IL-6, and IL-8 were statistically significantly higher in advanced stages of precancerous lesions as compared to early stages (P<0.05).(Tables 2, 3) The levels of serum and salivary TNF-α, IL-6, and IL-8 were also statistically significantly increased in oral leukoplakia, submucous fibrosis, and lichen-planus in contrast to normal healthy subjects. Serum and salivary correlation analysis revealed a strong and highly significant correlation for TNF-α, IL-6, and IL-8 levels in all groups as shown in Table 4.
IV. Discussion
Serum and salivary TNF-α, IL-6, and IL-8 were higher in advanced stages as compared to early stages of precancerous lesions and conditions, data which supports previous studies1415161718192021222324. TNF-α, IL-6, and IL-8 are potent angiogenic meditators with significant effects on tumor growth, and are associated with increased tumor vessel density and a worsened outcome15161718. Thus, these cytokines might act as surrogate biomarkers of angiogenesis and prognosis. It has been previously reported that excessive cell proliferation and activation of cellular actions can be instigated by chronic inflammation, which leads to the induction of irreversible DNA damage25. TNF-α, IL-6, and IL-8 released through the inflammatory response would promote tumor growth, while tumor growth further stimulates the inflammatory response, resulting in cyclic progression26. In the present study, serum and salivary TNF-α, IL-6, and IL-8 levels were upregulated in precancerous lesions and conditions. This finding is in line with most previous conducted work14151617, although one study has shown that salivary TNF-α and IL-6 were downregulated1819. This could be due to a small sample size and not using age- or gender-matched samples. Proinflammatory cytokine levels are elevated in submucous fibrosis due to immunoregulatory activity. Increased levels of NF-κB mediators might be associated with the development of oral precancerous and cancerous lesions. In the normal cell, stimulation of cytokines causes growth inhibition, while in oral cancer cells, stimulation of cytokines leads to upregulation of positive cell cycle regulators including NF-κB, signal transducers, and activators of transcription and the mitogen-activated protein kinase/extracellular signal-regulated pathway16. Upregulation of TNF-α, IL-6, and IL-8 might be protective in action.
Smoking is a risk factor of oral precancerous and cancerous lesions2. However, while smoking and chronic alcohol usage might be risk factors for cancer, this study showed no significant difference between controls and patients. TNF-α might act as an endogenous tumor promoter as well as an inducer of tissue remodeling required for tumor growth and spread22. IL-6 signaling has also been implicated in tumorigenesis23. TNF-α, IL-6, and IL-8 were also elevated in periodontitis patients21, but in the present study, subjects with periodontitis were excluded. So, the present study shows that the elevation of TNF-α, IL-6, and IL-8 is correlated with precancerous and cancerous lesions. Indeed, elevation of these cytokines in saliva might indicate the potential precancerous development into oral cancer22. Alternatively, these cytokines may be improperly produced in precancerous lesions, which could lead to induced growth, invasion, disruption of tumor suppression, and immune status. NF-κB activation leads to the upregulation of anti-apoptotic genes as a cell survival mechanism, by inducing physiological stress, which triggers an inflammatory response. In addition, NF-κB induces cytokines that regulate TNF-α, IL-6, and IL-8, which leads to the recruitment of leukocytes to the sites of inflammation27. There was good correlation between salivary and serum TNF-α, IL-6, and IL-8 in all groups. Since saliva can be easily collected, measurement of these biomarkers of diseases may prove useful in early detection of oral cancer risks. The salivary analysis for oral diagnosis may prove a cost effective method for screening large populations24.
Hence, salivary levels of NF-κB mediators were significantly elevated and may have diagnostic and prognostic utility as useful biomarkers for detection of precancerous and cancerous lesions. This study did not take into account factors such as diet, alcoholic history, and environmental factors, so further studies are required on large samples including these variables to determine the relationship between salivary biomarkers and oral cancer, and to further clarify their mechanism of action. It can only be concluded that patients with oral precancerous lesions have elevated salivary and serum cytokines compared to healthy controls and that the levels of salivary cytokines increase with the severity of dysplasia.

 XML Download
XML Download