

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
Condylar fractures account for 25%-35% of all mandibular fractures1. Mandibular condyles are anatomically susceptible to fractures because external force tends to focus on the region2. Such fractures cause occlusal dysfunction, temporomandibular joint (TMJ) dysfunction, mandibular movement dysfunction, and facial deformities; therefore proper treatment of condylar fractures is essential in preventing such problems.
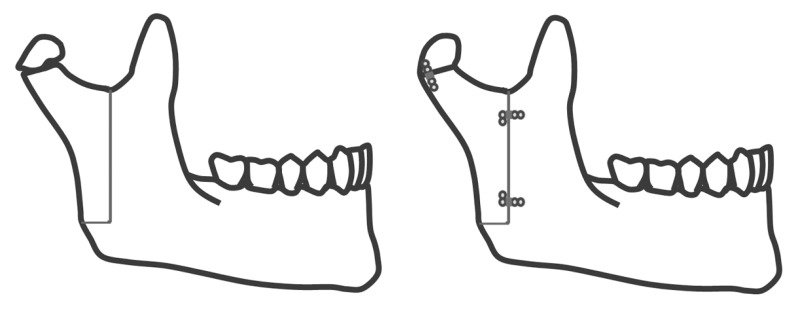
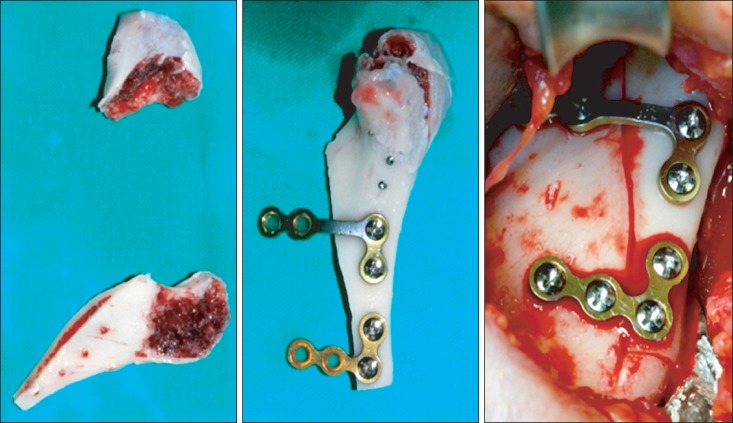
Treatment modalities are divided into two broad categories: conservative treatment and open reduction. Treatment choice depends heavily on the surgeon's preference and the selection criteria are still under debate. Those in favor of open reduction stress the importance of anatomical reconstruction and early recovery of mandibular function3,4,5. In 1983, Zide and Kent6 proposed guidelines for absolute and relative indications for open reduction. However in cases of superiorly positioned fractures with antero-medial displacement of condyle fragments, the standard approach can be difficult. Many studies report difficulty in access, visualization, fixation, and the dangers of harming nearby structures, such as the parotid gland or facial nerve7. Extracorporeal fixation utilizing vertical ramus osteotomy, first performed in 1981, could be a method to resolve these problems8.(Figs. 1, 2) Since then, a number of studies on extracorporeal fixation have been published9,10,11.
This study aims to compare and analyze mandibular condyle fracture patients treated with different modalities in order to assess the clinical application of extracorporeal fixation.
II. Materials and Methods
1. Patients
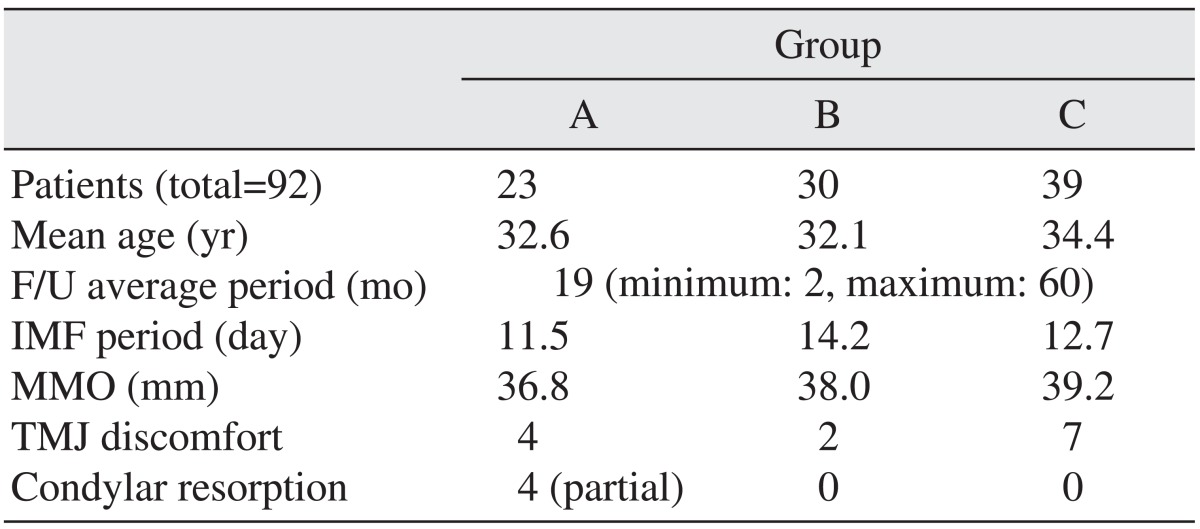
Among patients who visited at the Department of Oral and Maxillofacial Surgery in Sun Dental Hospital (Daejeon, Korea) for mandibular condyle fracture between January 2007 and September 2012, 92 patients (73 males and 19 females, 33.1±13.3 years of age) who had follow-up data available (minimum 2 months, maximum 60 months, average 19 months) were selected. The patients were divided into 3 groups: group A, treated by extracorporeal fixation (n=23, 18 males and 5 females); group B, treated by standard open reduction (n=30, 24 males and 6 females); and group C, treated with intermaxillary fixation only (n=39, 31 males and 8 females). Clinical and radiographic exams were performed on all of the selected patients. Of the 92 patients, 11 had bilateral condylar fractures. Seven of the bilateral condylar fracture patients were treated with conventional open reduction because of favorable fracture location and/or non-displaced fracture fragments. The other 4 patients were treated with extracorporeal fixation because of high fracture location and/or significant displacement of fracture fragments.
The inclusion criteria for open reduction are as follows: 1) inability to achieve occlusion with closed reduction, 2) invasion of the joint space by a foreign body or fractured bony segment, 3) decreased maximum mouth opening (MMO, under 30 mm) with or without mechanical locking, 4) severely displaced condylar fracture with disarticulation of the condyle from the glenoid fossa, and 5) loss of vertical dimension due to bilateral condylar fracture.
In some cases, conventional open reduction was converted to extracorporeal reduction during the procedure.
2. Methods
1) Clinical analysis
Patient treatment data such as surgical method, period of intermaxillary fixation, maximal mouth opening, and occurrence of TMJ disorder were collected from medical records. TMJ pain upon mandibular function was assessed through patient interviews.
2) Radiographic analysis
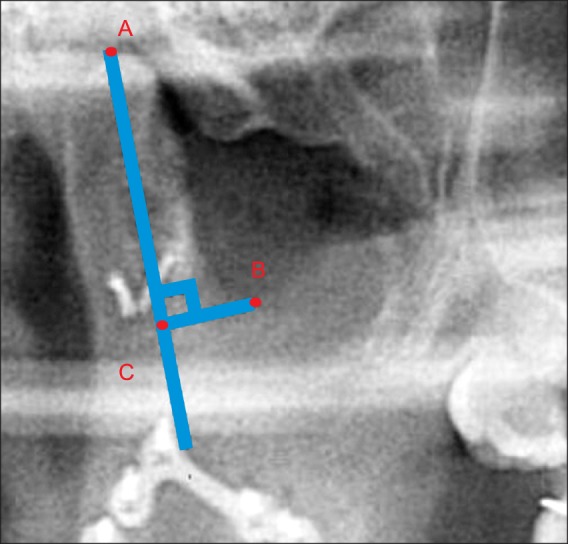
Preoperative, immediately postoperative, and follow-up panoramic X-rays were used to compare fracture sites and contralateral normal sites. A line was drawn from the superior-most point of the condylar head 'A' bisecting the condylar neck. From this line, a second perpendicular line to the inferior-most point of the mandibular notch 'B' was drawn, and the distance between the intersection point 'C' and 'A' were measured.(Fig. 3) This value was used to describe the amount of condylar head resorption on the fractured side, which was graded as severe (>2/3 of the normal condylar head), moderate (1/3-2/3), or mild (<1/3). Radiographic analysis was performed using ViewRex (Techheim Co., Ltd., Seongnam, Korea) software.
III. Results
1. Treatment selection in relation to patient age
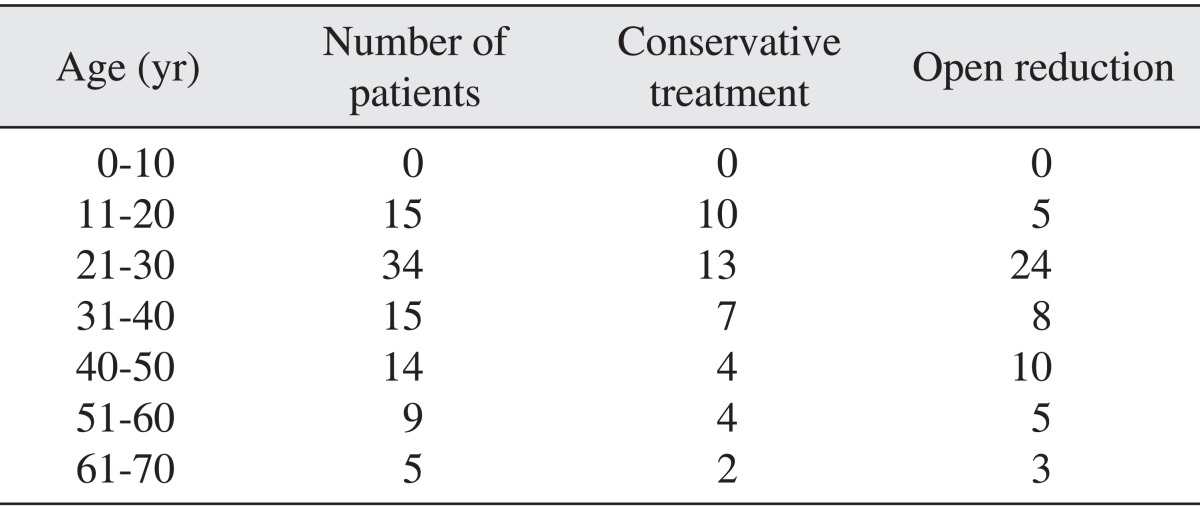
Conservative treatment was preferred for patients under 20 years. Table 1 shows the distribution of treatment choices according to patient age.
2. Treatment choices in relation to the location of the fracture and displacement of fragments
Conservative treatment was preferred for condylar head and condylar neck fractures. Extracorporeal fixation was used in condylar head and condylar neck fractures when medially dislocated fragments caused mechanical locking of the mandible. In condylar base fractures, the more inferior the position of the fracture and the further the fragment displacement, the more conventional open reduction was preferred. Condylar fractures were classified according to Lindahl's classification3.
3. Period of postoperative intermaxillary fixation
The average postoperative intermaxillary fixation period (group A) was 11.5 days, while the average fixation periods for open reduction patients (group B) and conservative treatment patients (group C) were 14.2 and 12.7 days, respectively.
4. Mandibular functional movement
1) Maximum mouth opening
Group A, B, and C patients had an average MMO of 36.8 mm, 38.0 mm, and 39.2 mm, respectively. Two patients in group A had a limited MMO of less than 30 mm.
5. Postoperative temporomandibular joint disorders
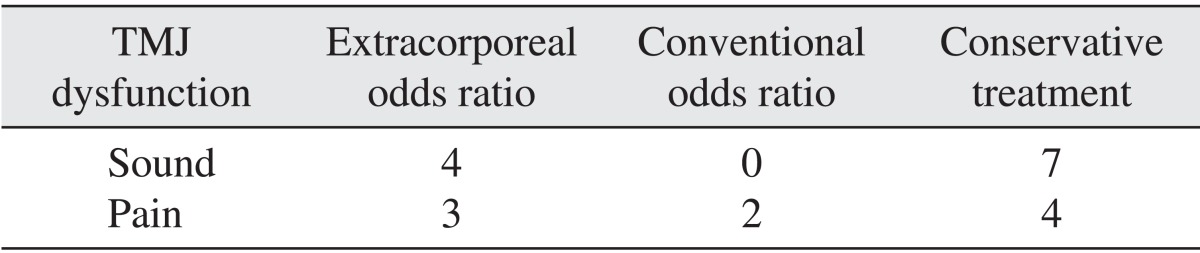
In group A, 4 of the 23 patients reported TMJ click, and 3 complained of pain along with click. None of the group B patients had TMJ click postoperatively, but 2 complained of pain. In group C, 7 of the 39 patients complained of TMJ click and 3 also complained of pain.(Table 2)
6. Radiographic analysis
In group A, 4 of the 23 patients exhibited moderate resorption (1/3-2/3) of the treated condylar head, and 3 of these 4 patients were advanced in age.(Fig. 4) The remaining 19 patients showed no resorption.(Fig. 5) There was a correlation between age and condylar resorption. Comminuted fractures demonstrated significantly higher condylar resorption compared with simple fractures (P=0.001). There were no significant differences between patients who had a short intermaxillary fixation (IMF) period (<2 weeks) and patients who had a long IMF period (≥2 weeks) (P=0.421). Condylar head fractures did not exhibit significantly higher condylar resorption than fractures in other locations (P=0.735). No group B or C patients demonstrated resorption of the condylar head. All results are shown in Table 3.
While conservative treatment was preferred in younger patients and those with smaller fragments or less fragment dislocation, open reduction was preferred in cases involving larger fragments and greater fragment displacement. MMO and lateral excursion movement increased in the following order: group A < group B < group C. However, since extracorporeal fixation was used in patients with larger fracture fragments and greater displacements, direct comparison of surgery outcomes has little significance. TMJ dysfunctions, such as click and pain, were not correlated with specific procedures. According to radiographic analysis, 4 patients in group A showed moderate condylar head resorption (1/3-2/3 of the condylar head). Condylar head resorption was not observed in patients in group B or C.
IV. Discussion
Mandibular condyle fractures are classified as intracapsular, extracapsular, or subcondylar according to the vertical location of fracture, and as undeviated, deviated, or dislocated according to the location of fractured fragments. Such classifications play an important role in treatment planning.
Numerous studies have evaluated the selection criteria for open reduction and conservative treatment of condylar fracture12,13,14. According to Eckelt's study15 comparing open reduction and conservative treatment, open reduction patients treated with interfragmentary screw (lag screw) fixation had better outcomes than those treated conservatively. Open reduction should always be considered, unless condylar fracture is incomplete or fragments are not displaced, as it allows for anatomical reconstruction and early functional recovery.
Zide and Kent6 reported that condylar displacement into the middle cranial fossa, an inability to reconstruct proper occlusion, and lateral luxation of the condylar head are absolute indications for open reduction. However, many clinicians and surgeons still seem to prefer conservative treatment. This is most likely due to the difficulty accessing and visualizing fracture sites using the conventional intraoral approach, and the risks the extraoral approach entails, such as harming critical anatomical structures (e.g., the facial nerve or intermaxillary artery). Recent advancements in fixation materials, endoscope technology, and surgical tools such as right-angle drills and drivers have made intraoral access and visualization more convenient, allowing for less invasive surgical procedures. Along with such technological advancements, indications for open reduction have grown broader than before.
Reduction of condylar fracture is more challenging when fractures are superiorly located and fragments are displaced. Moreover, in the case of unfavorable fractures, the medial pterygoid muscle pulls the fractured fragment of the condylar head antero-medially. According to Mikkonen et al.11, reduction of a medially displaced condyle fragment is very difficult using the submandibular approach, and detachment of the condylar head is sometimes required for satisfactory repositioning of this fragment because the lateral fragment can obstruct the surgeon's view and manipulation of the displaced medial fragment.
For treatment of superiorly located condylar fractures with medially displaced fragments, Nam8 introduced 'Nam's method', which includes vertical ramus osteotomy, extraoral reduction and fixation of the fractured condyle to the osteotomy fragment, and re-fixation of the ramus. This technique allows for anatomically accurate reduction of fragments. However, this extracorporeal fixation procedure requires detachment of all soft tissue from the medial fragment, including the blood supply, and the resulting complications are a major concern for many clinicians and oral surgeons.
Bell and Kennedy16 performed vertical ramus osteotomy on monkeys, detached all soft tissue from the medial fragment, and re-fixated the osteotomy fragment to the mandible. Resorption and deposition of bone tissue with formation of a new functional condylar head were observed. The newly formed condylar head, however, was composed of histologically abnormal tissue.
Daniels et al.17 performed free bone grafts and reported resulting histological changes.
Boyne9 reported significant condylar resorption in patients treated with extracorporeal fixation. In their study, condylar resorption occurred within the first 2 years of surgery and then remained stable for up to 15 years. Changes in occlusion were not observed9.
Mikkonen et al.11 published a follow-up study involving 9 male condylar fracture patients treated with extracorporeal fixation, and reported shortening and deformation of the affected condyles; however, nearly complete TMJ function was observed without any permanent complications.
In 2009, Gupta and Sahoo18 reported a 2-11 years follow-up study including 18 condylar fracture patients treated with extracorporeal fixation who experienced satisfactory occlusal stability and functional recovery. One of the 18 patients showed complete resorption of both condylar fragments, but recovery of occlusion and mandibular movement were satisfactory.
Davis et al.19 reported a success rate of 70% in a study involving 11 free graft procedures on 10 condylar fracture patients. Three patients experienced condylar resorption within 9 months.
In this study, 4 of 23 patients treated with extracorporeal fixation exhibited moderate condylar resorption within 6 months, but stabilized after that. All 4 cases involved comminuted fractures with medially displaced fragments, thus making rigid fixation using miniplates difficult.
Three patients with condylar resorption also had a short IMF period, ranging from 6 to 9 days.
In 2012, Adeyemi et al.20 reported earlier satisfactory healing in the patients with a long IMF period (4 to 6 weeks).
Condylar resorption is likely due to avascular necrosis related to detachment of soft tissue from the medial fragment medial fragment. While many studies on extracorporeal fixation report histologic changes, postoperative histologic analysis was not performed in this study because histologic samples were not attained from patients. Some studies reported mandibular dysfunction and TMJ disorder after the extraoral fixation method was used. Detachment of the TMJ capsule is the suspected cause of loss of function of TMJ ligaments and medial pterygoid muscle fibers in these cases. In spite of the moderate condylar resorption shown in some of the patients in the present study, there were no subjective complaints of TMJ pain or mandibular dysfunction. Further study on the fate of detached ligaments and medial pterygoid muscles is under way.
In all extraoral approach procedures, scar formation is of great interest to both surgeons and patients. There were no complaints related to scar formation in this study. This is likely due to the surgeon's esthetic considerations in choosing an appropriate approach site, meticulous procedure, and the use of medication to prevent scar tissue formation.
There is always the risk of facial nerve damage from extraoral approaches. While the location of facial nerve branches varies from patient to patient, knowledge of general anatomy and statistical data on the distribution of the facial nerve21, along with meticulous operative technique, should help prevent facial nerve-related complications. In this study, 3 patients showed signs of facial nerve weakness, but all of them recovered within 3 months of surgery.
V. Conclusion
In this study, TMJ ankylosis or complete resorption of the condyle did not occur after extracorporeal fixation. Therefore, if conventional open reduction and fixation of condylar fracture is difficult, extracorporeal fixation should be considered as an alternative treatment. Surgeons should also consider predictors of condylar resorption such as age and comminuted fracture when selecting appropriate treatment.


 XML Download
XML Download