

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
In 1652, Pietro Marchetti first described an elongated styloid process related to an ossifying process of the stylohyoid ligament. Eagle, an otolaryngologist, later defined Eagle's syndrome in 19371,2. Eagle considered any styloid process longer than 25 mm in an adult to be abnormal. He found that 4% of the population had elongated styloid processes, but only 4% of those with this trait had symptoms3-5. He divided the syndrome into two forms: classic type and carotid artery type.
The classic type of Eagle's syndrome can develop after tonsillectomy, when scar tissue under the tonsillar fossa compresses and stretches cranial nerves V, VII, IX, and X. This type includes symptoms such as foreign body sensation, pain referred to the ear, and dysphagia.
The carotid artery type of Eagle's syndrome presents with other symptoms, such as migraines, and neurological symptoms, caused by irritation of the sympathetic nerve plexus. If the internal carotid artery is compressed, then ipsilateral headaches can occur. If the external carotid artery is compressed, then there can be pain in the temporal and maxillary branch areas4,6.
Here, we report a rare case of the stylohyoid ligament bilaterally elongated to more than 60 mm in a 51-year-old female. We did a surgery by extraoral approach and patient's symptom was improved.
Go to : 
II. Case Report
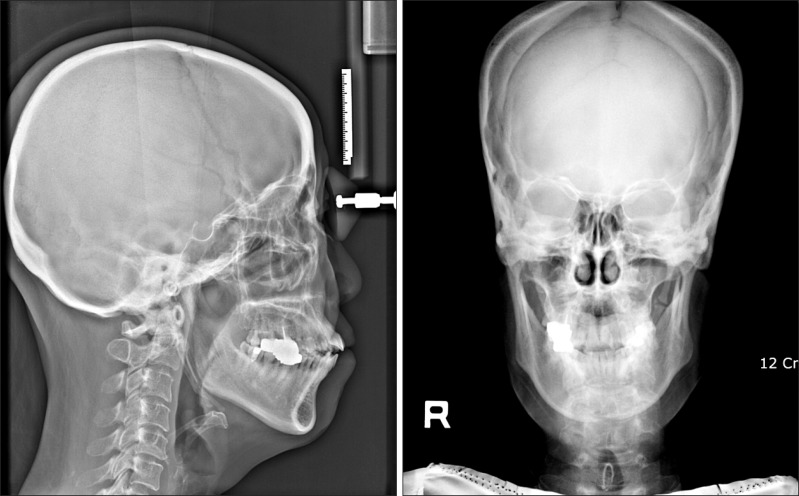
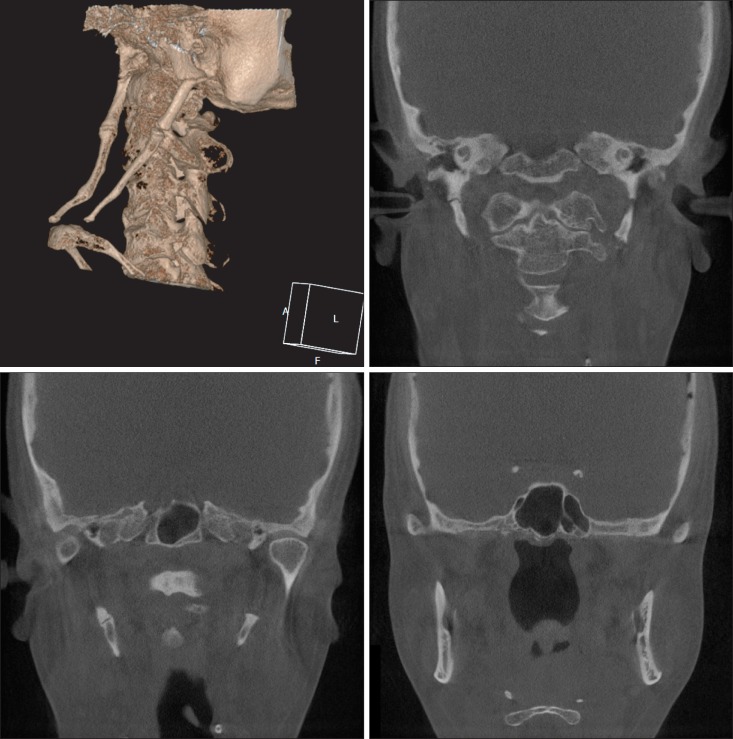
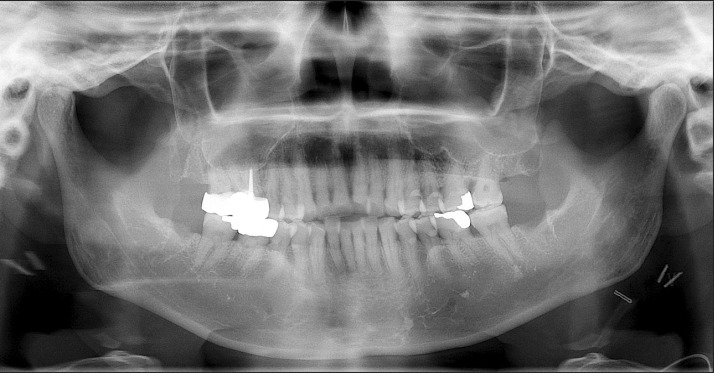
A 51-year-old female patient with throat pain and dizziness was referred to the Department of Oral and Maxillofacial Surgery at Kyung Hee University Dental Hospital in Korea. Upon turning her head, the patient felt facial swelling, dizziness, as well as neck and shoulder pain. She also had a sense of fullness in her neck. Her past medical history included a thyroid nodulectomy 1 year prior to presentation. During the clinical exam, we could not feel either stylohyoid ligament in the oral cavity. However after imaging, we could see that both ligaments were elongated in the panoramic view.(Fig. 1) Lateral cephalometry and reverse Towne projection film showed that the stylohyoid ligaments extended down to the hyoid bone.(Fig. 2) Using cone-beam computed tomography (CBCT), we determined that their lengths were more than 60 mm and their diameters were almost 5 mm at the thickest site, and the ligaments displayed a twig morphology.(Fig. 3)

We diagnosed this patient with Eagle's syndrome by clinical and radiographic exams. We planned for complete removal of both elongated stylohyoid ligaments using an extraoral approach under general anesthesia.
A horizontal incision was placed in a skin crease 5 cm inferior to the lower border of the mandible. A cervical incision was made from the proximal side of the sternocleidomastoid muscle to the hyoid bone, and the elongated stylohyoid ligaments were detached and the muscular attachments removed via subperiosteal dissection. We resected the ligaments and attachments using a rongeur forcep and small osteotome.(Figs. 4, 5) In addition, we extracted all of the wisdom teeth. The day after surgery, we confirmed that most of the elongated stylohyoid ligaments were removed using panoramic radiography and CBCT.(Figs. 6, 7) After resection, the patient's neck and shoulder pain and dizziness upon head movement disappeared, but she had discomfort with swallowing. She also complained that the skin around the surgical site was loose.



At the 3-month follow-up, we reevaluated the surgical site using panoramic radiography and CBCT. We determined that the patient's symptoms such as pain, dizziness, swollen feeling, and odynophagia had resolved. However, the patient still complained of loose skin around the surgical site.
Go to :
III. Discussion
The styloid process is derived from the second branchial arch of Reichert's cartilage. This cartilage consists of four components: 1) the tympanohyale, which arises from the periotic capsule of the temporal bone and is a process attached to the inferior surface of the petrous part of the temporal bone; 2) the stylohyale, which usually forms the greater part of the styloid process proper; 3) the ceratohyale, which forms the stylohyoid ligament; and 4) the hypohyale, which forms the lesser cornu of the hyoid bone7. The styloid process is an elongated tapered projection that originates in the petrous portion of the temporal bone, lying medially and anteriorly to the stylomastoid foramen, between the internal and external carotid arteries, and laterally to the tonsillar fossa. The stylopharyngeal, stylohyoid, and styloglossal muscles are attached to the styloid process. This bony process supports the stylohyoid and stylomandibular ligaments. The stylohyoid ligament connects the apex of the styloid process and the lesser horn of the hyoid bone, and the stylomandibular ligament extends from the styloid process to the parotideomasseteric fascia between the mastoid process and the mandible8.
Recently, Murtagh et al.9 presented three etiologic theories to explain the development of Eagle's syndrome. The first theory is congenital elongation of the styloid process due to the persistence of the cartilaginous precursor, the second is the calcification of the stylohyoid ligament by a mysterious process, and the third is the growth of osseous tissue at the insertion of the stylohyoid ligament. Steinmann proposed three mechanisms that might case ossification: 1) reactive hyperplasia, when trauma activates the remnants of the original connective and fibrocartilaginous cells; 2) reactive metaplasia, or an abnormal healing following a trauma that initiates ossification of the stylohyoid ligament; and 3) anatomic variance, which occurs without any distinctive trauma10. Camarda et al.11 proposed a fourth mechanism of aging developmental anomaly in the absence of apparent radiographic ossification.
Murtagh et al.9 explained that Eagle's syndrome symptoms stem from its pathophysiology, which includes: 1) the theory that traumatic fracture of the styloid process with a proliferation of granulation tissue is able to apply pressure on the surrounding area; 2) compression of the glossopharyngeal nerve, the mandibular branch of the trigeminal, or the chorda tympani; 3) the theory of insertion tendonitis due to inflammation of the tendinous part of the stylohyoid insertion; 4) irritation of the pharyngeal mucosa by direct compression or post-tonsillectomy scarring (with involvement of cranial nerves V, VII, IX, and X); and 5) the theory of irritation of the sympathetic nerves surrounding the carotid vessels9.
Diagnosis is guided by the clinical history and physical and radiographic examinations. The physical examination consists of palpation of the tonsillar fossa and local infiltration anesthesia. Transpharyngeal palpation demonstrates a bony projection and reproduces the characteristic pain. Symptom relief should follow anesthetic injection in the tonsillar fossa. Radiologic evaluation, such as panoramic radiography, lateral cephalometry, Towne projection film, or CT, may be used. In the panoramic view, the styloid process is visualized posteriorly to the external acoustic meatus with a descendant and anterior trajectory. When elongated, it attains over one third of the length of the mandibular ramus. CT allows for the precise measurement of the styloid process length, direction, and anatomic variance, in addition to evaluation of stylohyoid ligament ossification8.
Eagle's syndrome can be treated nonsurgically and surgically. A pharmacological approach includes transpharyngeal infiltration of steroids or anesthetics into the tonsillar fossa. In addition, there are two surgical approaches, intraoral and extraoral. In the intraoral approach, the styloid process is found with palpation of the tonsillar fossa. The overlying mucosa and superior constrictor muscle are incised vertically, and the styloid process are dissected out and resected using a rongeur forcep. If necessary for exposure, a standard tonsillectomy should be performed first. The intraoral approach is good for aesthetic consideration as external scarring is avoided and for shorter operative times. Nevertheless, exposure of the retropharyngeal spaces to intraoral contents increases the infection risk. The intraoral approach also has the disadvantages of poor access, as in cases of trismus, and risk of intraoperative injury. An extraoral approach involves making a cervical incision from the proximal portion of the sternocleidomastoid muscle to the hyoid bone, and then dissecting and removing the styloid process. The external approach has the advantage of good anatomic exposure of the styloid process. However, it requires more intervention and results in a visible scar3,12.
In this case, we planned surgical excision because the patient's symptoms were severe. As both elongated stylohyoid ligaments were quite large, we resected using an external approach. We also extracted 4 wisdom teeth. The resected stylohyoid ligaments measured more than 60 mm long, as indicated in the CT scan. After surgery, the patient's symptoms improved but a scar remained. At the 3-month postoperative follow-up, the patient's symptoms were further decreased although some discomfort remained.
Go to :
 XML Download
XML Download