

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
As societies continue to be urbanized, changes have been observed including more centralized populations, increased traffic due to industrialization, and increased opportunities to enjoy sports and other leisure activities. These changes not only affect people's lifestyle but also increase the rate of injury. Therefore, research on maxillofacial injury and fracture has been actively conducted in various fields.
The maxillofacial region is prone to injuries and fractures due to its protruding anatomical feature. The frequency of fracture around the mandibular region is higher than that of the other parts of the body1-3. Although maxillofacial fracture may not be life-threatening, immediate treatment should be applied because fractures can directly affect functional aspects and the appearance of the maxillofacial region. According to domestic and international research on mandibular fracture, car accidents, assaults, and external injuries are classified as main etiologic factors of mandibular fracture. The research period, regional characteristics, and socioeconomic levels affect the etiologic factors, and can cause differences in the pattern and distribution of fracture1,2,4-6. Therefore, periodical case analysis and statistical research help confirm the tendency of mandibular fractures and allow researchers to develop new and effective precautionary measures.
Results of patient mandibular fractures treatment by open reduction and internal fixation was retrospectively analyzed. The analysis was based on age, gender, seasons, types of fracture, and etiologic factors during the eleven years between 2002 and 2012. This study was conducted at the Department of Oral and Maxillofacial Surgery in Kyung Hee University Dental Hospital.
II. Materials and Methods
The purpose of this study was to analyze the results of maxillofacial fracture in 735 patients, who were received open reduction operations and internal fixation to treat mandibular fracture. The patients were operated on under general anesthesia by members of the Department of Oral and Maxillofacial Surgery in Kyung Hee University Dental Hospital from January 2002 to December 2012. Continuous monitoring and statistical categorization were conducted in this study based on medical records and patient radiographs.
III. Results
1. Occurrence distribution ratio by gender, age, and time period
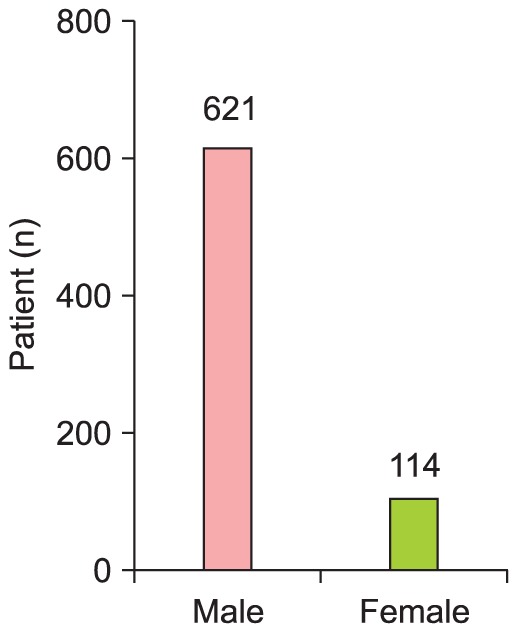
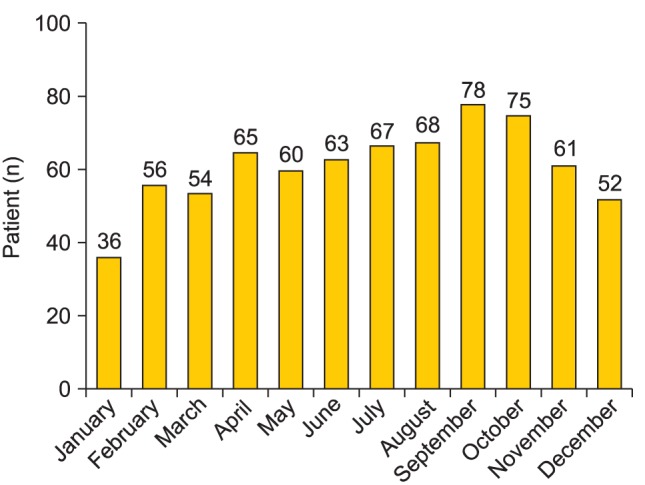
Among 735 patients, 621 patients (84.5%) were male, and 114 patients (15.5%) were female. The ratio of males to females in the patient group was 5.45 : 1.(Fig. 1) The most affected age group was the 20s, with 280 patients (38.1%), followed by early adolescents and teenagers with 152 patients (20.7%), and patients in their 30s, with 136 patients (18.5%). The month of September was associated with the greatest number of injuries, with 78 patients, while January had the least number of injuries, with 36 patients. By seasons, autumn (September, October, and November) had 214 patients (29.1%), and winter had the fewest number of patients, with 145 total patients (19.7%).(Fig. 2) The average number of annual injuries was 66.8 patients. However in 2007, the greatest number of injuries was in 78 patients, and in 2005 the least number of injuries, with 51 patients, was observed.(Fig. 3)
2. Cause
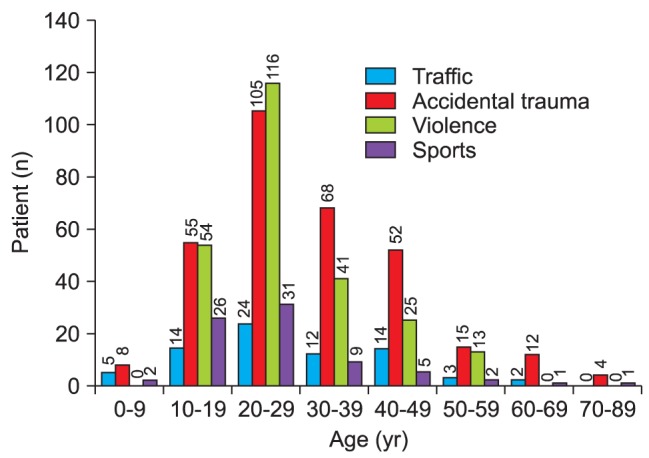
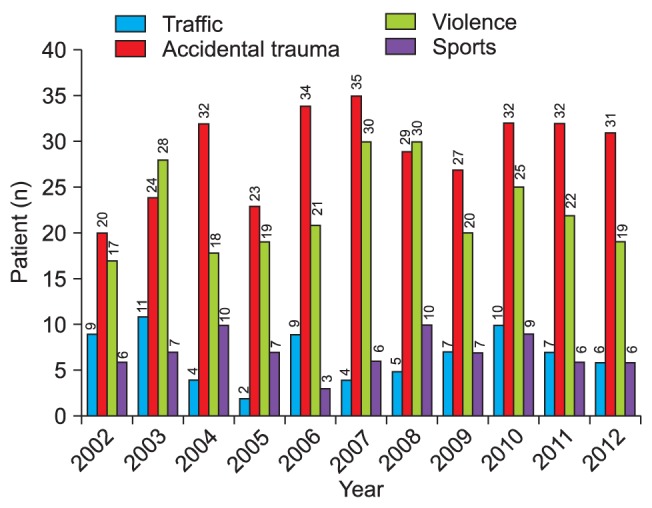
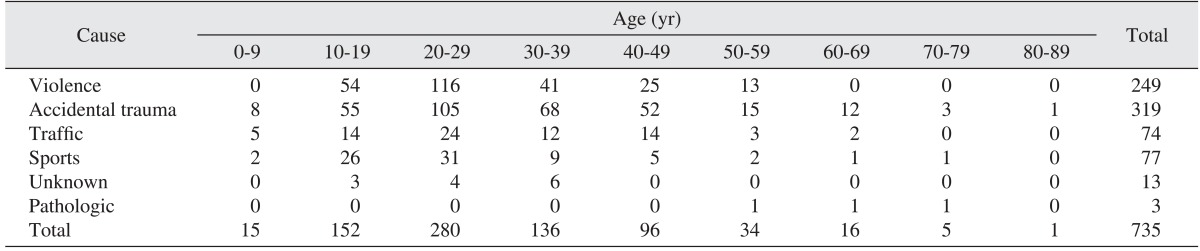
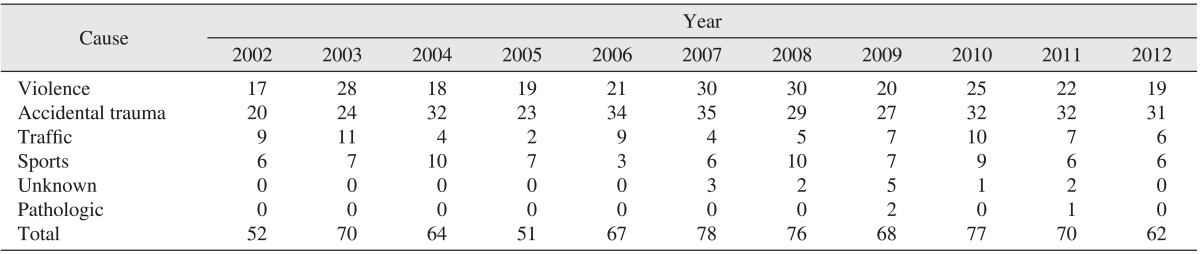
Three hundreds and nineteen patients (43.4%) were injured because of daily-life activity such as falling and collision, which was the highest cause of trauma among all the etiologic factors. Fracture caused by violence was rated second with 249 patients (33.9%), followed by sport activity with 77 patients (10.5%), car accidents with 74 patients (10.1%), and unknown factors with 13 patients (1.8%). Three patients (0.4%) reported with fractures induced by pathological causes. By age group, physical assault was the main etiologic factor of fracture in patients in their 20s, but external injury was the most common factor in the rest of the age groups.(Table 1, Fig. 4) Physical assault caused the most fractures (40.0%) in 2003, but daily-life activity-associated fractures were the most common occurrences.(Table 2, Fig. 5)
3. Fracture part frequency and distribution
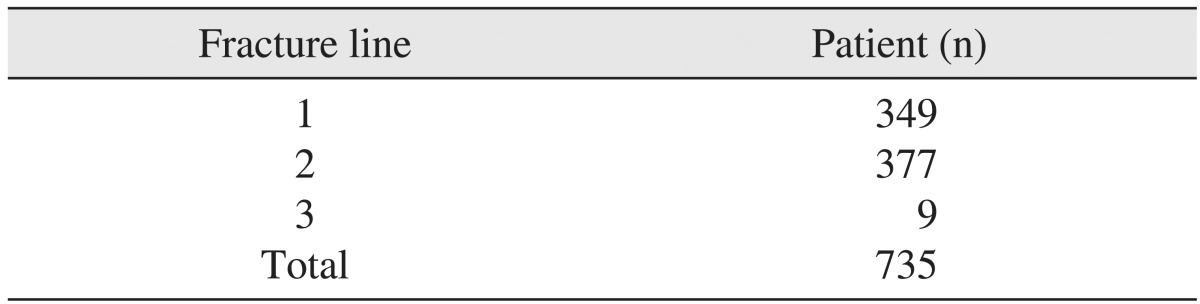
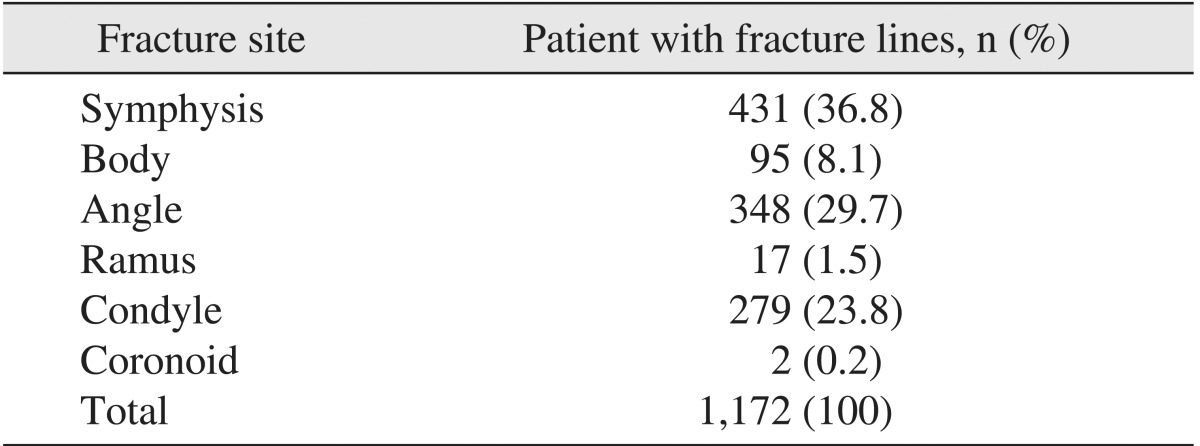
Among 735 patients, 1,172 fracture lines were observed. On average, there was about 1.6 fracture line per person. The patients who had a single fracture line was 349 (47.5%), and there were 377 patients (51.3%) with two fracture lines and 9 patients (1.2%) with three fracture lines, respectively.(Table 3) Symphysis fractures were the most frequent and were identified in 431 patients (36.8%). There were 348 patients (29.7%) with an angle fracture, 279 patients (23.8%) with a condyle fracture, 95 patients (8.1%) with a body fracture, 17 patients (1.5%) with a ramus fracture, and 2 patients (0.2%) with a coronoid process fracture.(Table 4, Fig. 6)
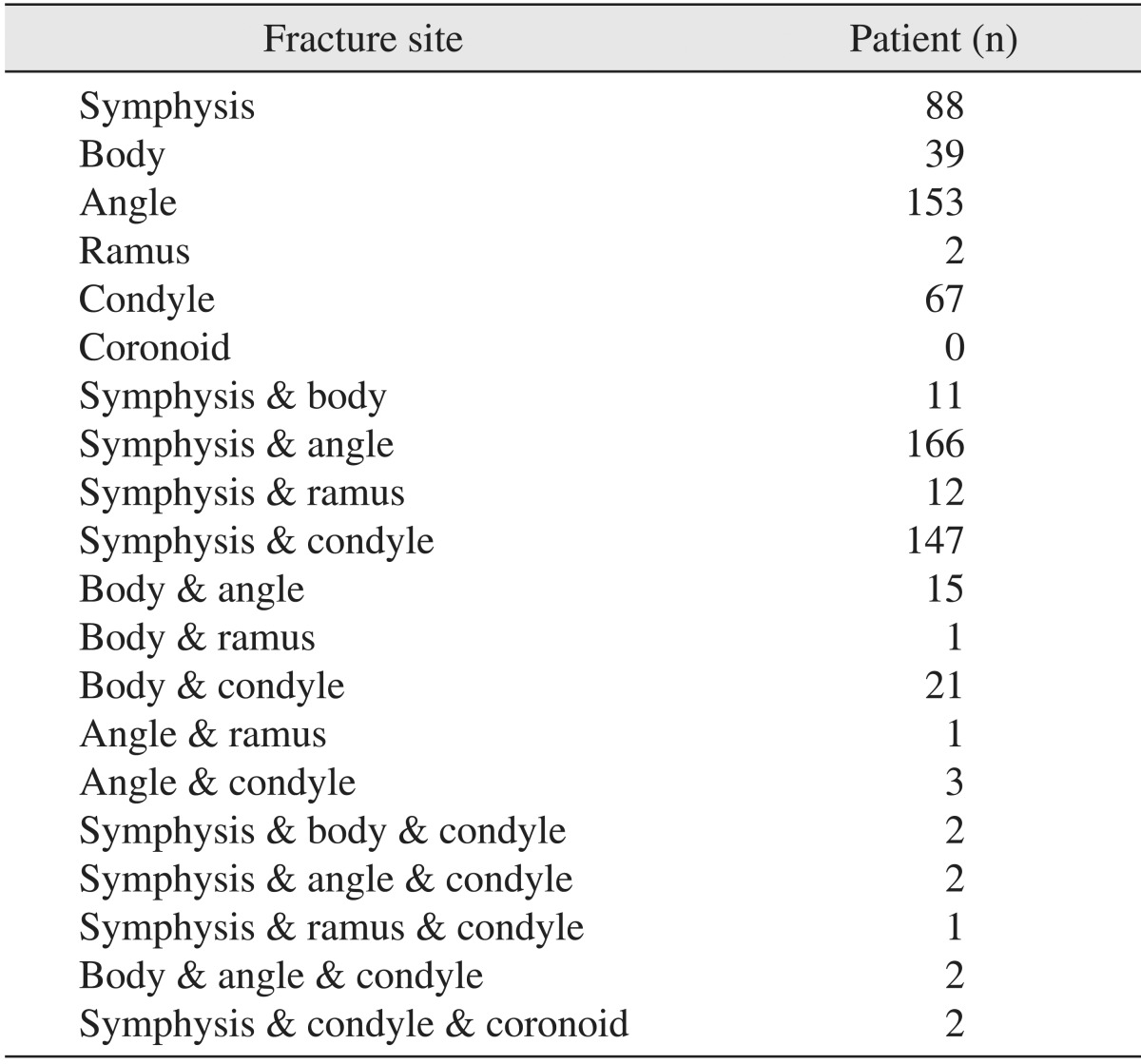
Regarding single fractures, angle fractures were most prevalent and were identified in a total of 153 patients (20.8%). There were 88 patients (12.0%) with a symphysis fracture, 67 patients (9.1%) with a condyle fracture, 39 patients (5.3%) with a body fracture, and 2 patients (0.3%) with a ramus fracture, respectively.
Analysis of patients with multiple fractures indicated that there were 166 patients (22.6%) with symphysis and angle fractures and 147 patients (20.0%) had symphysis and condyle fractures. Additionally, there were 21 reported patients (2.9%) with body and condyle fractures, followed by 15 patients (2.0%) with body and angle fractures, 12 patients (1.6%) with symphysis and ramus fractures, 11 patients (1.5%) with symphysis and body fractures and 3 patients (0.4%) with angle and condyle fractures. One patient with a body and ramus fracture and one patient with an angle and ramus fracture (0.1%), respectively, were identified.(Table 5)
The results indicated that 249 patients were injured because of etiologic factors associated with physical assaults. Among the 249 patients, 74 patients (29.7%) had symphysis and angle fractures, followed by 58 patients (23.3%) with angle fractures, 48 patients (19.3%) with symphysis and condyle fractures, and 22 patients (8.8%) with a symphysis fracture. A fracture line was identified in 142 patients (57.0%), especially in cases that presented with angle fractures. Additionally, 103 of the 142 patients had fracture lines on the left side, and the remaining 39 patients (27.5%) had fracture lines on the right side.
IV. Discussion
The etiologic factors of facial fracture are variable and depend on regional and social characteristics as well as time periods. Many research reports have cited car accidents, external injuries, sports activities, and assaults as main etiologic factors of fractures4-6. As socioeconomic development progress and the quality of life improves, these changes also affect etiologic factors. Lifestyle, economic development, and different subject groups also impact study results and affect the type and distribution of fractures that are reported.
Incidental collision or falling were the most common cause of fractures in this study. Other research reports showed similar results7. Assaults were the second most common factor while car accidents showed a relatively lower ratio with 74 patients (10.1%). However, other studies have reported that car accidents were the most common etiologic factor in mandible fractures, therefore, regional characteristics could have affected the differences in these results1-5,7-9. This study was based at a hospital located near a residential area with a densely-concentrated population, in addition to close proximity to universities with a number of social restaurants and bars and the traffic system and conditions may have impacted the results.
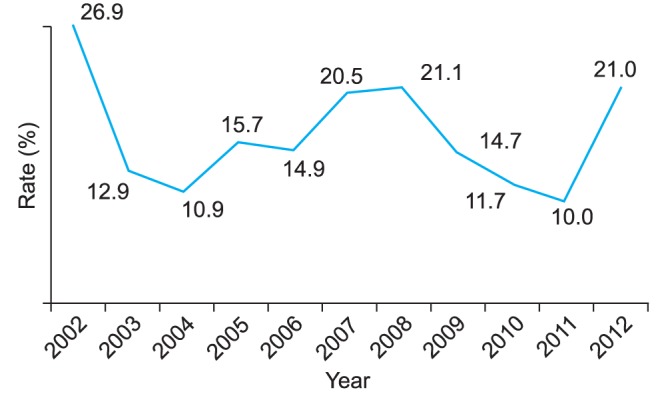
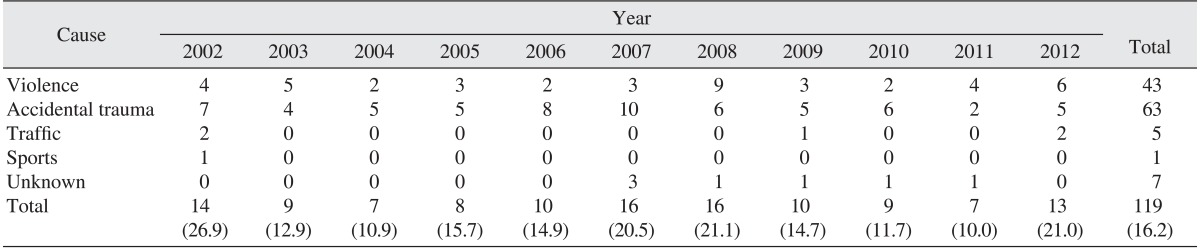
Analysis indicated that 10.0%-26.9% of fractures were related to alcohol consumption (Fig. 7), and of these cases, 43 of 249 patients (17.3%) incurred fractures from assaults, 63 of 319 patients (19.7%) were hospitalized for external injuries and 13 patients were classified with unknown causes.(Table 6) Another report also concluded that 17.8%-41.4% of fracture cases were related to alcohol1,5,8,10. The degree of injury was more severe when an individual was injured under the influence of alcohol11,12.
Additional studies have reported a high proportion of external injuries related to alcohol consumption and assaults were reported as the major reason for fracture10-12. However, some cases may have not recorded alcohol consumption that was related to the cause of fracture. This may be omitted for several reasons including patient reporting and patient history recording by physicians and if accounted for, the number of cases and incidence of alcohol consumption-related fractures could increase4. Research conducted at Kyung Hee University between 1985 and 199013 and this research reported that external injuries, assaults, and car accidents were the most common etiologic factors of fracture. However a previous study reported 25.3% of patients with car accidents, and sport activities with 4.2% of patients. In this report, car accidents were reported with 10.1% of fractures and sports activities were reported in 10.5% of cases.
These results showed that the fracture ratio by car accidents decreased, but the fracture ratio by sports activity increased, based on the population in this study. The ratio of male to female patients was 5.45 : 1 and fractures occurred more frequently in male patients. This finding was similar to results from other domestic and international studies4-7. The months of September and October showed the highest fracture frequencies and the month of January was the lowest. This distribution appeared to be related to the frequency of outdoor activities and social events, according to seasons. Annually, 61 patients on average were hospitalized due to fracture during the eleven year study period, with similar seasonal distributions. Patients in their 20s had the highest recorded incidence of fractures. External forces such as falling and collision and physical assaults were the most common etiologic factors of fractures and were prevalent in patients that were in their 20s.
An average of 1.6 fracture lines per person was observed when the frequency and regional occurrence pattern of mandible fractures were analyzed. Out of all of the patients, 52.2% (384/735 patients) presented with two or more fracture lines.
Regional fractional line pattern analysis indicates that when an external force is applied to the mandible region, the symphysis, which protrudes due to anatomical positioning, will be affected first. The symphysis is the most affected region in cases of mandible fracture, which is attributable to the anatomical position. Additionally, the mandible angle region has the second highest fracture frequency. When applied external force travels from the anterior to posterior position, the mandible angle, which is relatively thinner than other regions, is subject to damage. The condyle is the third affected area due to its posterior position within the mandible and its location at the center of the skull, where the applied external force is finally concentrated.
In cases with single fractures, the mandible angle is the most common fracture region followed by the symphysis and condyle. The symphysis and angle were the most common sites of multiple fractures followed by the symphysis and condyle. This finding was similar to other research studies6,7,13. Based on reports from other studies, the mandible angle fracture was the most frequent in cases of single fractures13, especially with assault-related fractures, and the symphysis and angle fractures were most common in multiple fractures5. Bilateral comparison indicated that the left side had a fracture distribution ratio of 72.5% (103/142). Although fracture patterns have not changed recently, compared to previous research studies6, some changes have occurred in the etiologic factors that affect fractures. Most fractures are caused by accidents and alcohol consumption is highly correlated with etiologic factors of mandibular fractures. Therefore, developing guidelines and preventative measures for mandibular fractures could include addressing controllable factors such as drinking.
V. Conclusion
This study evaluated and analyzed clinical and statistical data of patients who were treated with open reduction and internal fixation for mandible fractures at the Department of Oral and Maxillofacial Surgery in Kyung Hee University Dental Hospital between 2002 and 2012. The following results were summarized in this study.
The frequency distribution indicated that the male to female ratio was 5.45 : 1, which showed a higher prevalence in male patients.
Patients in their 20s were the most affected age group, which was followed by 10s and 30s.
The most common etiologic factors of mandible fracture were external injuries, assaults, sports activities, and car accidents, respectively.
The frequency ratio of fractures associated with alcohol consumption was 10.0%-26.9%.
On average, 1.6 fracture lines per person were observed, and the symphysis was the most affected region followed by the angle and condyle.
The ratio of multiple fractures with two or more fracture lines was 52.5%, the symphysis and angle was the most affected site followed by the symphysis and condyle.


 XML Download
XML Download