

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
Clear cell odontogenic carcinoma (CCOC) is a rare jaw tumor that was first described by Hansen et al.1 in 1985, in which patients presented with local bony invasions without metastasis. At first, CCOC was called a clear cell odontogenic tumor or clear cell ameloblastoma, and was considered more aggressive than ameloblastoma. The potential for CCOC to metastasize was initially unclear; however, CCOC was defined as a benign tumor in the 1992 World Health Organization (WHO) classification2.
The WHO reclassified CCOC as a malignant tumor of odontogenic origin in 20053 because of its aggressive and destructive growth capacity and metastasis to the lungs and lymph nodes4,5,6,7,8. About onethird of CCOC cases were initially misdiagnosed, and the primary diagnosis was ameloblastoma which lead to inadequate treatment for some patients. In this case report, we describe a case of a CCOC, which presented in a similar manner to a cystic lesion; the patient was misdiagnosed and received insufficient treatment. We introduce this case to discuss differential patient presentations to reduce the rate of malignancy misdiagnosis.
II. Case Report
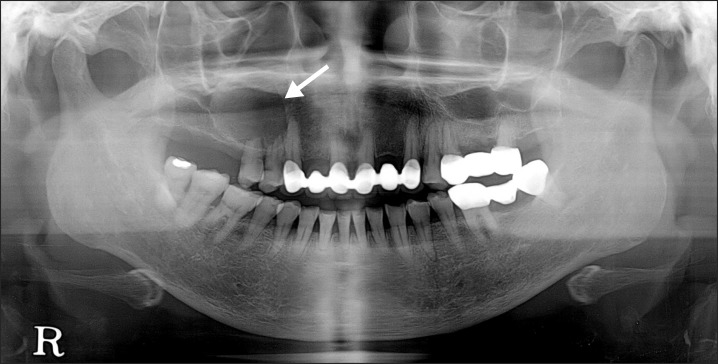
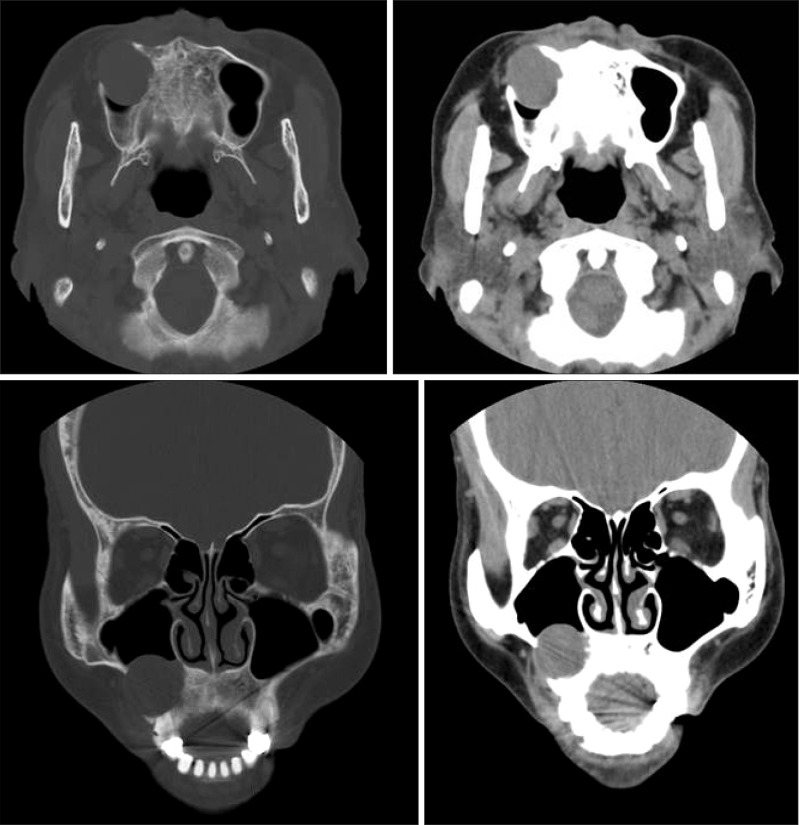
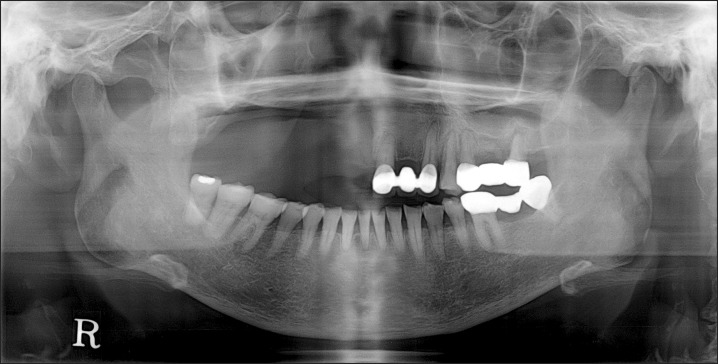
A 66-year-old female visited the Department of Oral and Maxillofacial Surgery at Yonsei Dental Hospital due to swelling and pain on the right premolar maxillary area. Incision and drainage had been performed at a local clinic 5 days previously. Clinical examination showed fluctuating swelling on the right maxillary vestibule with tenderness to palpation, severe tooth mobility and loss of vitality on the first and second premolars and no appreciable cervical lymphadenopathy. A panoramic radiograph revealed an approximately 27×29 mm well-defined radiolucency in the apex of the maxillary right premolars with root resorption.(Fig. 1) A computed tomography (CT) scan showed a low attenuated cystic lesion with a volume of 7,419 mm3 (Simplant software; Materialise, Leuven, Belgium).(Fig. 2)
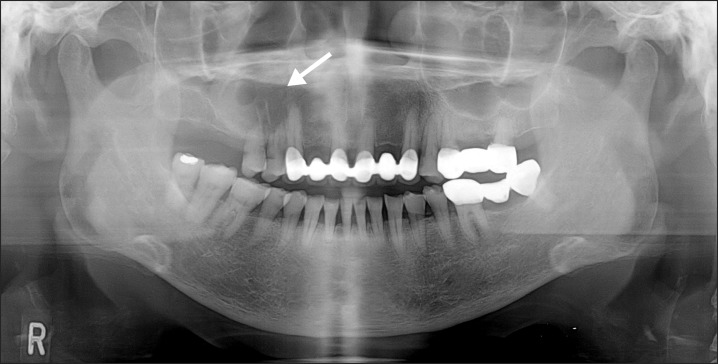
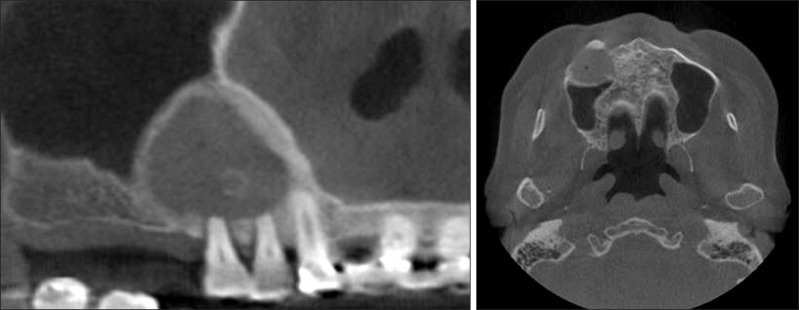
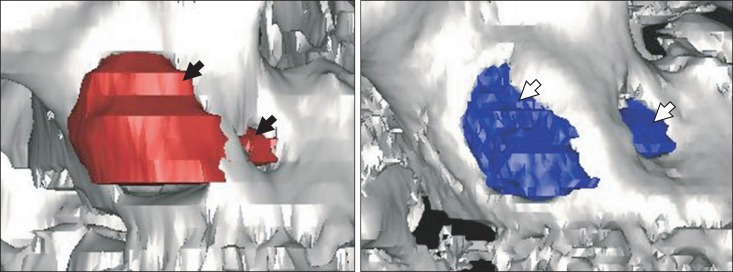
At first, the lesion was diagnosed as infected odontogenic cyst (radicular cyst), the patient received decompression in order to separate the cyst from maxillary sinus wall. A yellowish exudate was discharged from the cyst while a local anesthetic was injected. The cystic wall was too thin and fragile to be sent for pathologic examination. Two months after decompression, a panoramic radiograph showed that the lesion size was reduced to approximately 25×26 mm.(Fig. 3) The lesion was reduced to a volume of 4,797 mm3 (Simplant software) on the 3-month follow-up conebeam CT.(Fig. 4) The measurement and comparison may not be precise because of the differences in CT imaging; however, there was definite shrinkage of the lesion.(Fig. 5)
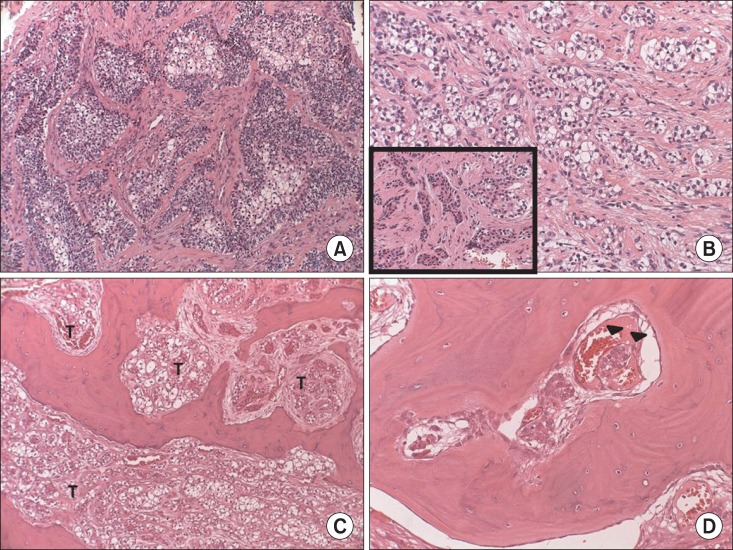
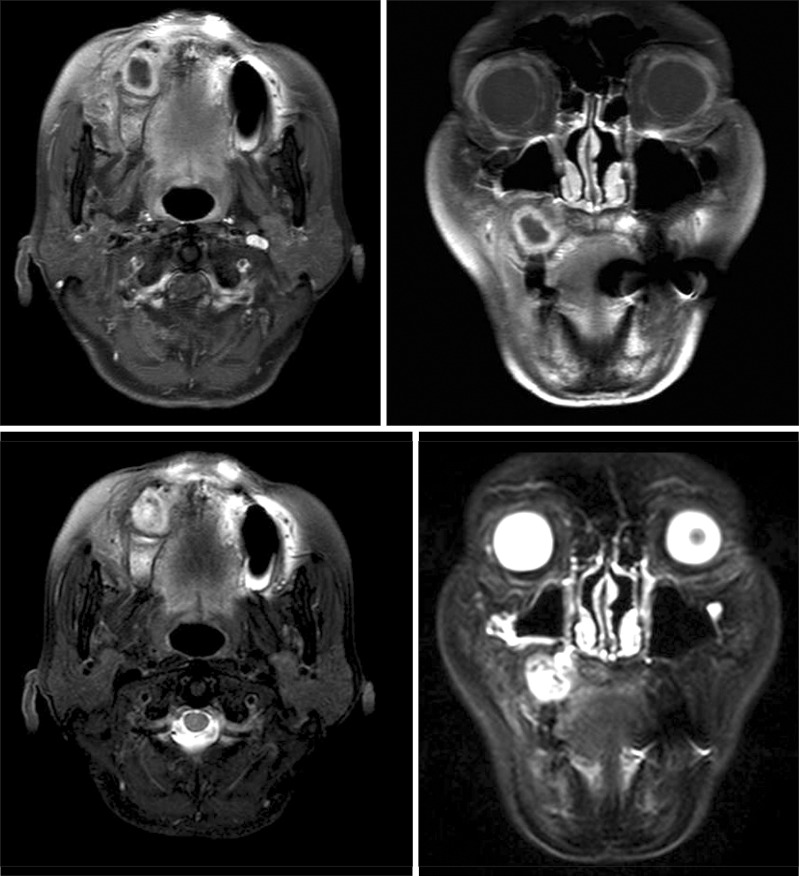
Because there was not a change in the lesion size, a cyst enucleation was performed and specimens were sent to oral pathology. Unexpectedly, the pathologic results indicated that the mass was CCOC.(Fig. 6. A, 6. B) Magnetic resonance imaging of the neck and positron emission tomography CT, were taken to examine the lymph nodes and distant metastasis.(Fig. 7) There were no pathologic lymph nodes and evidence of metastasis. A partial maxillectomy was performed without neck dissection. An obturator was placed at the time of surgery and a 2.4×2.0 cmsized CCOC with a positive basal resection margin, massive bone marrow infiltration and lymphovascular permeation was reported.(Fig. 6. C, 6. D)
Postoperative radiotherapy was conducted 1 month after surgery. No recurrence or metastasis was detected 10 months after the surgery.(Fig. 8)
III. Discussion
Nearly 100 cases of CCOC have been reported in the Englishlanguage literature to date, and these tumors have a higher reported incidence in females with an male/female ratio of 1 : 1.8. Most cases of CCOC have been diagnosed in patients over the age of 40, with an average age of 54 years. The mandible is more frequently involved than the maxilla, and the posterior of the jaw is a more frequent site than the anterior site9,10,11.
Radiographic findings show mainly radiolucent lesions with or without regular margins, although some cases exhibited a mixed radiolucent-radiopaque lesion. Previous reports have suggested that painless swelling was the most common clinical symptom. In addition, tooth mobility and pain were occasionally associated as symptoms9,10,11.
Approximately one half of patients that were diagnoses with CCOC experienced a recurrence. The likelihood of the recurrence depended on the method of initial therapy and the extent of the tumor invasion. Three-quarters of the patients who were treated with conservative care (curettage or enucleation) had recurrence and onethird of the patients who were treated with resection experienced a recurrence. Conservative care (curettage or enucleation) and presence of soft tissue involvement were associated with a higher recurrence rate10,12. The ideal treatment approach for CCOC has not been determined. A wide resection with at least 1 cm of a tumor-free margin is recommended and when there is evidence broad soft tissue invasion, palpable neck lymph node, perineural invasion or tumor removal without free margins, adjuvant neck dissection and/or radiotherapy should be considered10,12,13. However, except for squamous cell carcinoma and high-grade central mucoepidermoid carcinoma, neck dissection is rarely required for maxillary carcinomas without nodal metastases12,13,14.
In our case, the patient had swelling, incision and drainage history and a well-defined unicystic radiolucent lesion, that was comparable with a cystic lesion. At first we misdiagnosed the lesion as an infected cyst, performed decompression and were unable to send specimen for pathologic examination. Our treatment was limited because we did not make a correct diagnosis when the patient first presented at our clinic. When decompression was performed, the clinical findings were similar to a cystic lesion and during follow the up period we found that lesion size decreased. Currently, mass properties have not been described in previous reports, and our case study presented with both radiographic and clinical similarities to cystic lesion symptoms; for these reasons our diagnosis was delayed. Additional reports have indicated that many cases of CCOC are misdiagnosed because of its rarity and similarity to cystic lesions11,13. In this report, we discuss a patient that presented with a painful cystic lesion, jaw enlargement jaw and loosening teeth. Similar cases should be considered for the possibility of malignant CCOC to identify and treat patients with CCOC.
 XML Download
XML Download