

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
Sinus membrane perforation is one of the most common complications to occur during sinus-bone grafts. Perforations are classified according to their size: small (5-10 mm) or large (>10 mm)1. For a small perforation, closure with a collagen membrane or other biomaterial is recommended1,2,3. For large perforations, it is recommended to stop the surgery and perform an additional surgery after the perforation is fixed. Newly introduced repair methods for large perforations include local flaps, collagen membranes, or autogenous block-bone grafts4,5. Herein, we report 8 cases in which a large perforation in the sinus membrane was closed with a pedicled buccal fat pad graft6. A buccal fat pad is an autogenous graft material that has been widely used as an alternative method for the repair of small-sized intraoral defects caused by oral and maxillofacial surgeries. This study was conducted to assess the clinical prognosis and long-term changes for bone grafts that were performed simultaneously with repair of large sinus membrane perforations using a pedicled buccal fat pad.
Go to : 
II. Cases Report
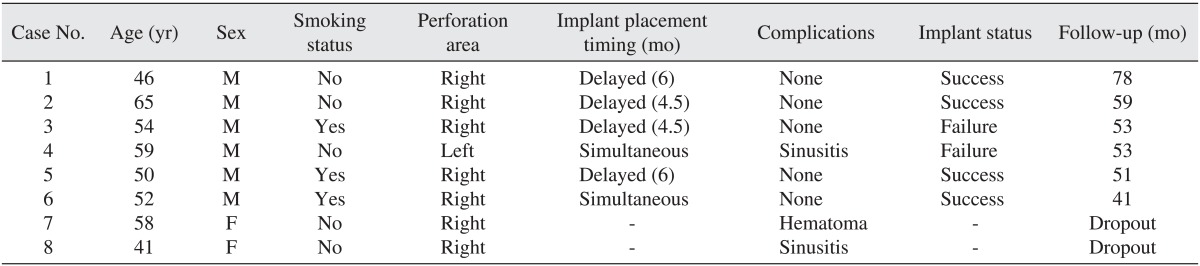
From among the patients for whom a perforation larger than 1 cm developed during sinus membrane elevation from January 2004 to December 2007, those for whom the reconstruction was performed using a pedicled buccal fat pad were selected for this study. Eight patients were included. The ages of the patients ranged from 41-65 years, with an average age of 53. Six patients were male, and two patients were female. The perforation area was located in the right maxillary sinus in seven cases, and the left maxillary sinus in one case. Four patients had systemic diseases, such as diabetes, hypertension, or bronchial asthma, all of which were well controlled with medications.
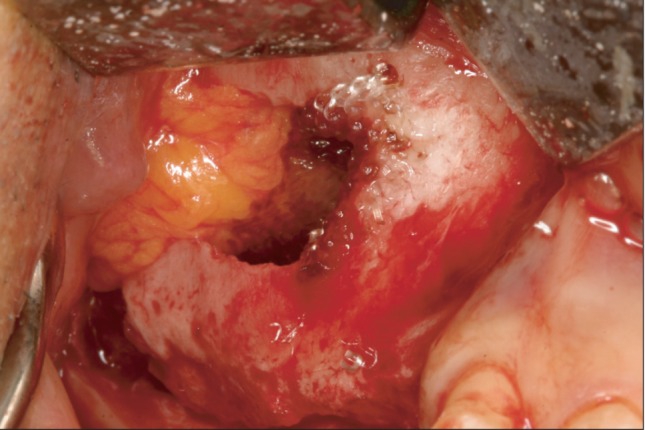
All patients received surgery while under general anesthesia. After performing a crestal incision and a mucoperiosteal flap elevation, the lateral wall of the sinus becomes exposed. During the process of forming an oval bony window using a round bur, the membrane is elevated and perforations larger than 1 cm were able to develop. We exposed a pedicled buccal fat pad on the inside of the mucoperiosteal flap by performing a blunt dissection toward the posterior, superior, and lateral directions using a curved hemostat.(Fig. 1) By moving the perforation area to the sinus roof area, we partially closed it while it was in a tension-free state. We also performed additional closures of the internal perforation area by inserting a resorbable collagen membrane (Ossix Plus; OraPharma, Louis Drive Horsham, PA, USA). For bone-graft materials, we used a mixture of autogenous bone and allogenic bone (OrthoBlast II; Stryker Orthobiologics, Kalamazoo, MI, USA) and/or xenogenic bone (Bio-Oss; Geistlich Pharma, Wolhusen, Switzerland). Block bones and particulated bones that were harvested from the ramus and the maxillary tuberosity were used for autogenous bones. Four patients received a bone graft only during the primary surgery, and 4-6 months later, implants were placed secondarily. Two patients received their implants and bone graft simultaneously. The remaining two patients received only a bone graft and follow-up observation was terminated early.
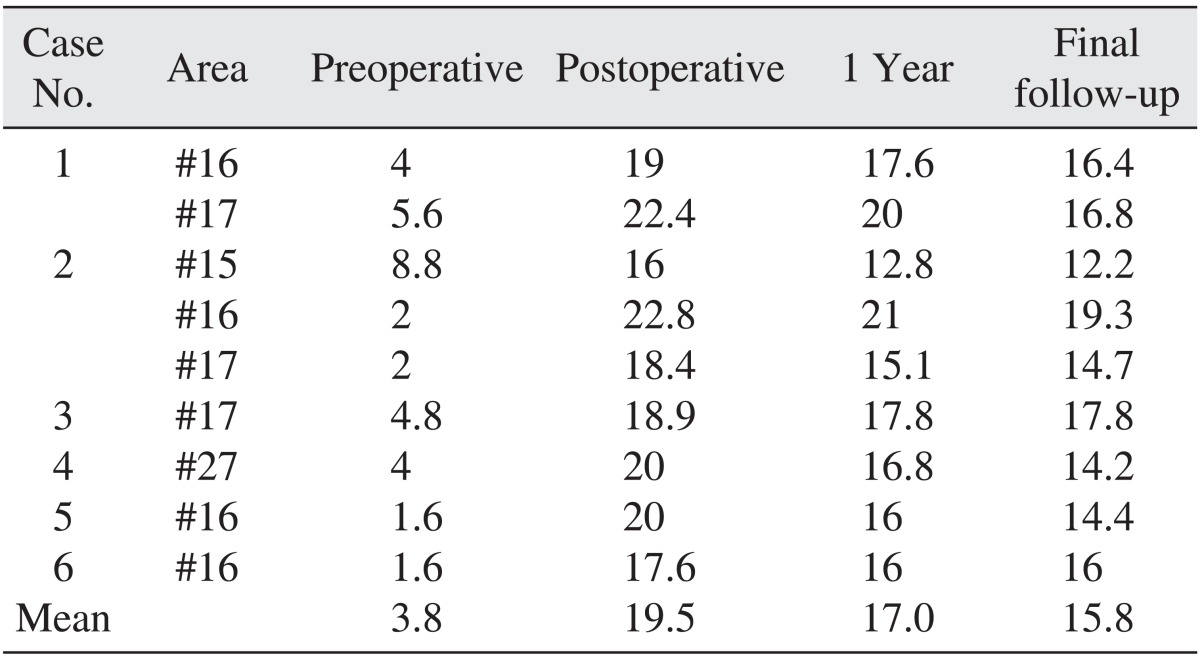
We examined, the postsurgical complications, treatment procedures, and the outcomes from each implant. The follow-up observation period after sinus-bone graft ranged from 41-78 months, with an average of 56 months. Follow-up was terminated early for two patients. Using panoramic radiographs, we measured bone height at three time points: preoperatively (residual bone), immediately postsurgery, and at final follow-up. The preoperative height of remaining alveolar bone was measured from the crest to the sinus floor. To document any increases in bone height, the postoperative measurement was taken from the alveolar crest of each implant to the topmost part of the sinus-bone graft. The magnification of the radiograph was measured and evaluated based on the length of each implant. The panoramic radiographs taken one year after surgery and at the final follow-up were used to measure the volume of resorbed graft material.(Fig. 2)

1. Case 1
A right maxillary sinus bone graft was performed in a healthy 46-year-old male patient. Residual alveolar bone height was about 4-6 mm. A large perforation occurred during sinus membrane elevation. The perforation was closed using a pedicled buccal fat pad and a collagen membrane and the sinus was grafted using a block bone from the mandibular ramus and xenogenic bone (Bio-Oss). The postoperative alveolar bone height was about 19-23 mm. No specific postoperative complications appeared. Two implants were installed at areas #16 and #17 six months after the graft surgery. A final prosthesis was installed an additional six months later.(Fig. 3)

2. Case 2
A right maxillary sinus bone graft was performed on a healthy 65-year-old male patient. The residual alveolar bone height was about 2-9 mm. The sinus was grafted using a mandibular ramus block bone and Bio-Oss. No specific postoperative complications arose and three implants were installed in areas #15, #16, and #17, four and half months later. An additional six months later, a final prosthesis was installed.(Fig. 4)

3. Case 3
A right maxillary second-molar extraction and right sinus-bone graft were performed on a 54-year-old male patient who was diagnosed with diabetes mellitus but was in good condition; he was also a smoker (one pack of cigarettes per day). His residual alveolar bone height was 4.8 mm. Bone chips of maxillary tuberosity, Bio-Oss, and OrthoBlast II were grafted at the site. The patient healed well with no sinusitis. After approximately four to five months, one implant was installed at area #17. After eight months, the second operation was performed but osseointegration was not successful. Therefore, the implant was removed and replaced simultaneously. The implant was successful and a permanent prosthesis was installed after another eight months.(Fig. 5)

4. Case 4
A left maxillary sinus-bone graft and a simultaneous implant placement at area #26 were performed on a 59-year-old male patient. The residual alveolar bone height was 4 mm. Although the patient had bronchus asthma and hypertension, he remained in good condition. We used a mandibular ramus-block bone, Bio-Oss, and OrthoBlast II, as our bone graft material. The height of the alveolar bone increased to 20 mm after surgery. Two weeks after the operation, left rhinorrhea and fluctuant swelling occurred. Maxillary sinusitis was diagnosed, and we treated it with incision and drainage, followed by a course of antibiotics; subsequently, all infection symptoms abated. Two months after the operation, the implant began to shift and was removed. We placed another implant two months later, and a permanent prosthesis was installed 14 months after the bone graft. However, even the permanent implant began to shift 51 months after its installation. The implant was removed, and another implant was re-installed at area #27: the alveolar bone height after this prosthesis was 14.2 mm.(Fig. 6)
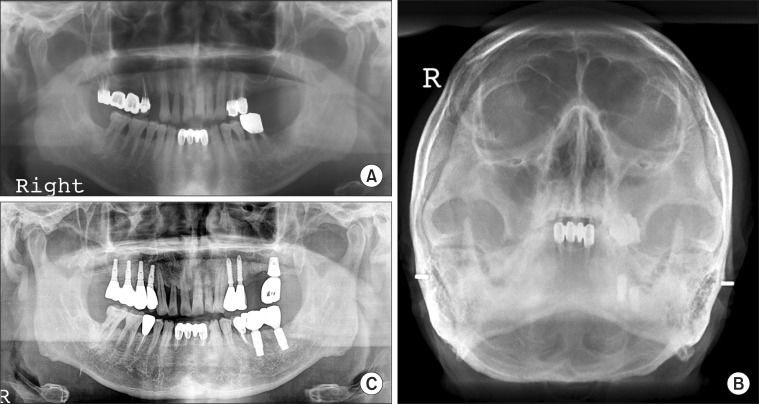 | Fig. 6Change in alveolar bone height (Case 4). A. Preoperative panoramic radiograph. B. Water's view two weeks after bone graft: left maxillary sinusitis developed. C. Panoramic radiograph 53 months after sinus bone graft: the second molar implant was removed and a new implant was placed at a distal area. The first molar implant was also removed.
|
5. Case 5
A right maxillary sinus-bone graft and delayed implant placement were performed on a 50-year-old male patient with diabetes mellitus who remained in good condition. He was also a smoker (1.5 packs per day). His residual alveolar bone height was 1.6 mm and bone chips of maxillary tuberosity, Bio-Oss, and OrthoBlast II were grafted to the site. No specific complications appeared. One implant was installed at area #16 six months later. A final prosthesis was installed after a six-month healing period; alveolar height after this period was 16 mm.
6. Case 6
A right maxillary sinus-bone graft and simultaneous implant placement were performed on area #16 in a 52-year-old male patient with hypertension who was in good condition. This patient smoked one pack of cigarettes per day. The residual alveolar bone height was 1.6 mm and the bone-graft material was a mixture of maxillary tuberosity bones, Bio-Oss, and DBX. No specific complications arose. A permanent prosthesis was installed eight months after the grafting operation.
7. Case 7
A right maxillary sinus-bone graft was performed on a healthy 58-year-old female patient. A bone graft was performed using a maxillary tuberosity, Bio-Oss, and DBX. Although a severe hematoma developed after the operation, this symptom abated over time. Implant placement and prosthodontic treatment were performed in a local clinic.
8. Case 8
A right maxillary sinus bone graft was performed in a healthy 41-year-old female patient. A mucous retention cyst was exposed and a large sinus membrane perforation occurred. The sinus was grafted with maxillary-tuberosity bone, Bio-Oss and OrthoBlast II. Two weeks after the operation, the patient complained of tenderness when she touched the right side of her nose and of nasal-obstruction symptoms. Therefore, we suspected a case of sinusitis and performed incision and drainage. There was a thick pus discharge in the sinus cavity, so we performed a pus culture and an antibiotic-sensitivity test. Sinus irrigation was performed daily. A two-week course of minocycline was prescribed. The patient's infection symptoms abated completely two weeks after we performed incision and drainage. At this point, the follow-up observation period ended.
A total of 12 implants were placed, three of which failed to osseointegrate in two patients. We removed the failed implants and replaced them with wider implants, and after a healing period, the prosthetic treatments were completed.(Table 1) Among the case patients, the average height of the preoperative residual bone from the sinus floor was 3.8 mm; this height increased to 19.5 mm immediately after surgery, decreased slightly to 17.0 mm one year after surgery, and was 15.8 mm at the final follow-up visit.(Table 2, Figs. 2, 3)
Go to :
III. Discussion
Reported rates of sinus membrane perforation during graft surgery range from 0%-58%7,8,9. Risk factors for perforation include greater height of residual bones, having a large edentulous area, presence of a septum, maxillary sinus lateral wall thickness, maxillary sinus mucosal thickness, smoking, presence of cystic lesions in the maxillary sinus, and previous maxillary allergy10,11,12,13,14. Ardekian et al.10 found that when the height of the residual bone to the maxillary sinus floor is low, risk of perforation increases. In cases where the residual bone height was less than 3 mm, an 85% perforation rate was reported. In cases where the residual bone height was 6 mm, the perforation rate dropped to 25%.
When the size of the perforation is very small (approximately 1-2 mm), the space can be closed by lifting the mucosa and overlapping it with the perforation. However, if the perforation is greater than 2 mm wide, it is better to close the perforation area using absorbable biomaterials, tissue adhesives, or platelet-rich plasma (PRP) gel15. It is well established that risk of bone-graft material loss and implant failure is higher in cases with a perforation complication than without14,16.
The clinical significance of sinus perforation is controversial. Hernández-Alfaro et al.17 examined the incidence of maxillary sinus perforation during maxillary sinus lifting and evaluated a variety of treatment methods. Among 474 cases of maxillary sinus elevation, sinus perforations occurred in 104 cases (25.15%). The perforation cases included a total of 272 implants, of which 247 were successful (90.91%). As the perforation area became larger, the success rate of implants decreased.
Many authors have reported that sinus perforations do not affect the complication rate after bone graft surgery18,19, but Proussaefs et al.20,21 reported that even if the perforated mucosa was repaired, new bone formation and the success rate of the implants decreased. Also, Schwartz-Arad et al.22 reported that maxillary sinus perforations were strongly associated with the development of other complications, such as postsurgical infections or cysts. Nevertheless, studies have shown that maxillary sinus perforations or postsurgical complications did not strongly influence the implant survival rate1,2,3,4,5.
The buccal fat pad (BFP) is special fat tissue that differs from subdermal fat. Anatomically, the BFP is easy to harvest during the course of dental surgery. In 1802, Bichat identified and described BFP. Since Egyedi23 used a pedicled buccal fat pad (PBFP) to close an oroantral fistula and an oronasal fistula in 1977, it has been widely used as an alternative method for the reconstruction of small- to medium-sized intraoral defects during oral and maxillofacial surgery24. Kim and colleagues6,25 reported successful results from using PBFP to cover a denuded bony surface during primary palatorrhaphy and in the reconstruction of large sinus membrane perforations. The excellent clinical outcomes from using PBFP, including rapid epithelialization and a high success rate, are partially due to its rich blood supply, which it gets from the maxillary, superficial temporal, and facial arteries. PBFP has many other advantages, including less necrosis and absorption than fat-free grafts. Furthermore, preoperative chemotherapy and postoperative radiotherapy did not seem to jeopardize survival of the graft, although these treatments do delay epithelialization26.
We repaired several large sinus-membrane perforations that developed during graft surgery using a PBFP and collagen membranes; we simultaneously performed a bone graft with a mixture of autogenous bone and other bony substitutes. In this study, the change in volume of the sinus bone graft was measured and we established that repneumatization developed slowly. At the time of follow-up (after an average of 56 months, postsurgery), sinus-bone volume decreased by an average of 3.9 mm. Two implants failed to osseointegrate in a 59-year-old male patient who developed sinusitis after surgery. The implants required removal and, although healing of the residual sinus-bone graft was eventually achieved, greater sinus-bone graft loss was noted during his final follow-up visit.
Large membrane perforations that develop during sinus-bone grafting can be reconstructed immediately using a PBFP graft and resorbable collagen membrane. Implants can be placed simultaneously with the bone-graft surgery or after a certain healing period, depending on the residual bone height. The height of the transplanted bone graft material shows a steadily decreasing pattern slowly over time. Based on this case series, we can confirm that the transplanted bone graft materials provide sufficient support for the implants.
Go to :
 XML Download
XML Download